

 , Pitak Laokirkkiat 1, Somsin Petyim 1, Isarin Thanaboonyawat 1, Japarath Prechapanich 1, Pavarit Humart 1, Patcharaporn Teammak 1, Nichamon Parkpinyo 1,*
, Pitak Laokirkkiat 1, Somsin Petyim 1, Isarin Thanaboonyawat 1, Japarath Prechapanich 1, Pavarit Humart 1, Patcharaporn Teammak 1, Nichamon Parkpinyo 1,*
1 Department of Reproductive Medicine, Faculty of Medicine, Siriraj Hospital, Mahidol University, 10700 Bangkok, Thailand
Abstract
Endometrial thickness is a key factor in determining the suitability for embryo transfer (ET) and influences the success of assisted reproductive technology (ART) outcomes. The aim of this study is to compare endometrial thickness in patients undergoing frozen-thawed embryo transfer (FET) who received platelet-rich plasma (PRP) injections alongside standard estrogen therapy with those receiving standard estrogen therapy alone.
In this randomized controlled trial (RCT), a total of 30 infertile women from Siriraj Infertility Clinic undergoing FET were enrolled and randomly assigned to three groups. Group 1 (PRP-1 group) received a single intrauterine PRP instillation on day 8 (D8) of the cycle prior to ET; Group 2 (PRP-2 group) received two intrauterine PRP instillations on D8 and D10 before ET; and Group 3 (Control) received standard estrogen therapy alone. Endometrial thickness, chemical pregnancy rate, clinical pregnancy rate, abortion rate, and cycle cancellation rate were recorded.
The mean differences in endometrial thickness on D8 and D12 were compared. The PRP-1 group showed the greatest increase in endometrial thickness compared to the other groups; however, the difference was not statistically significance (1.52 ± 1.10 in PRP-1, 0.72 ± 0.72 in PRP-2, 1.43 ± 0.88 in the Control group; p = 0.153). Chemical pregnancy rates were comparable across groups, with 33.34% in PRP-1 group and 42.85% in the control group. Similarly, clinical pregnancy rates were 16.67% in PRP-1 group and 42.85% in the control group; (p = 0.790 and p = 0.585, respectively). However, the cancellation rate was significantly higher in the PRP-2 group (77.78%, p = 0.015).
Single intrauterine PRP instillation on D8 prior to ET in a frozen-thawed cycle may improve endometrial thickness, although without statistical significance. In contrast, repeated PRP administration was associated with a higher cycle cancellation rate.
The study has been registered on https://clinicaltrials.gov/ (registration number: NCT06234540; registration link: https://clinicaltrials.gov/study/NCT06234540?cond=NCT06234540&rank=1).
Keywords
- PRP
- platelet rich plasma
- endometrial thickness
- thin endometrium
- refractory endometrium
- IVF frozen thaw cycles
The global total fertility rate (TFR) has been declining, reaching 2.2 live births per woman in 2024, down from 3.3 in the 1990s, and is projected to fall to 1 by 2050 [1]. This decline poses a significant challenge globally, prompting public health organizations to actively promote assisted reproductive technologies (ART) as a viable solution.
Among the various ART options, in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI) are the most widely used techniques, with success rates ranging from 35% to 40%, depending on the treatment center. These success rates are influenced by multiple factors, including the physiological condition of the patient and the clinical practices employed [2]. One critical factor affecting outcomes is endometrial thickness, which plays a significant role in the implantation process and overall outcomes of IVF/ICSI treatments [2, 3]. A deeper understanding of these variables is essential for improving IVF/ICSI success rates and addressing infertility worldwide.
A thin endometrium (less than 7 mm during the mid-cycle or anovulatory phase) is
associated with poor pregnancy outcomes [4], including reduced implantation
rates, lower pregnancy rates, and increased miscarriage rates [5]. While an
endometrial thickness of at least 8 mm is generally considered optimal for embryo
transfer (ET), several studies suggest that a thickness of
Although women diagnosed with a thin endometrium often receive hormone therapy to increase endometrial thickness according to standard protocols, alternative approaches also exist. These include increased estrogen doses, low-dose anticoagulants, vitamin E supplementation, sildenafil to enhance uterine blood flow, and treatments involving granulocyte-colony stimulating factor (G-CSF) injections. However, thin endometrial conditions may persist, resulting in the cancellation of ET during IVF cycles [5, 8]. This can cause increased financial and psychological stress for couples experiencing infertility [9].
Platelet-rich plasma (PRP) has emerged as a promising therapeutic approach, with research indicating its potential to enhance endometrial thickness and improve blood supply in women with a thin endometrium [9]. A 2015 study by Chang et al. [10] found that PRP not only increased endometrial thickness but also showed a trend toward improved pregnancy rates. This effect is likely due to PRP’s ability to increase cell proliferation, promote cell regeneration, and repair damaged cellular components [8]. These mechanisms are driven by growth factors and cytokines present in PRP, including vascular endothelial growth factor (VEGF), platelet-derived growth factor (PDGF), transforming growth factor (TGF), and insulin-like growth factor-1 (IGF-1) [4, 11]. Western blot analyses have shown that VEGF levels in PRP are up to 2.4 times higher than in plasma, while PDGF levels are up to 2.8 times higher, both differences being statistically significant (p = 0.030 and p = 0.001, respectively) [12].
Additionally, studies on both human [12] and murine [13] endometrial tissues have shown that PRP injection into the uterine cavity increases the expression of Homeobox A10 (HOXA10), a key marker of endometrial receptivity for embryo implantation. These studies also reported elevated Ki67 expression, indicating enhanced proliferation of glands and stroma in the endometrial tissue. Such histopathological findings further support PRP’s potential to improve endometrial receptivity. Moreover, the PRP preparation process is straightforward, and neither the plasma nor platelet components have been found to cause adverse effects [9, 14]. Due to its safety and efficacy, PRP has been widely applied across various medical fields, including the treatment of hair loss (alopecia), the reduction of inflammation and joint pain, and cosmetic procedures for skin rejuvenation [8].
In reproductive medicine, several studies have explored the application and optimization of PRP for infertility treatment, investigating its effect on both the endometrium and ovaries. However, results remain inconsistent, and a standardized protocol to optimize ART outcomes has yet to be established. For example, a 2022 study by Dogra et al. [8] measured endometrial thickness every 48 hours, administering PRP as needed until the thickness reached 7 mm. Their findings showed a significant increase in endometrial thickness following PRP administration in women with a history of cycle cancellation, with an average increase of 1.07 mm in fresh IVF cycles and 0.83 mm in frozen embryo transfer (FET) cycles [8]. In contrast, a 2020 study by Aghajanzadeh et al. [9] found no significant changes in endometrial thickness, implantation rate, clinical pregnancy rate, ongoing pregnancy rate, or miscarriage rate among women with recurrent implantation failure (RIF) submitted who received PRP 48 hours before ET. However, no prior studies have conducted a direct comparative analysis of the effects of a single PRP injection versus repeated PRP injections on endometrial thickness.
This study aims to evaluate the potential effects of PRP in enhancing endometrial thickness in women with a thin endometrium. Specifically, we compare endometrial thickness in patients undergoing FET across three groups: those receiving a single PRP injection with standard estrogen therapy, those receiving repeated PRP injections with standard estrogen, and those receiving standard estrogen therapy alone. As a secondary objective, we compare chemical pregnancy rates, clinical pregnancy rates, ongoing pregnancy rates, abortion rates, and cycle cancellation rates among the groups.
A single-blind, randomized controlled trial (RCT) was conducted. Inclusion
criteria were Thai women aged 18 years and older undergoing ET in a frozen-thawed
cycle with a history of ET cancellation due to thin endometrium (
Endometrial thickness was measured using transvaginal ultrasonography on days 3,
8, 12, and 14 (D3, D8, D12, and D14) of the menstrual cycle. Endometrial
thickness was measured with a 5 MHz vaginal transducer with the TOSHIBA Xario 100
TUS-X100 (Toshiba Medical Systems Co., Ltd., Otawara, Tochigi, Japan). All
measurements were performed by the same experienced operator (intra-observer
variation of
On D3, participants underwent a baseline ultrasound and were prescribed Estradiol hemihydrate (Estrofem®, Novo Nordisk Limited, Basel, Switzerland) at 2 mg orally, three times daily (6 mg/day) for five days.
On D8, participants with an endometrial thickness
On D12, participants with an endometrial thickness
For PRP preparation, 15 mL of peripheral blood was collected into Anticoagulant Citrate Dextrose Solution, Solution A (ACD-A) tubes (Lot No.: MFG 20230526; Shandong Hygeia Medical Packing Technology Co., Ltd., Rizhao, Shandong, China). The blood was processed using a Thermo Scientific™ Labofuge™ 400 Centrifuge (Thermo Electron Corporation, Karlsruhe, Germany) with a two-step centrifugation protocol: an initial spin at 1800 rpm for 12 minutes to separate red blood cells, followed by a second spin at 3400 rpm for 7 minutes to isolate PRP. Approximately two-thirds of the supernatant were discarded, and the remaining one-third (about 1 mL) was carefully mixed using a sterile pipette before being loaded into a syringe for intrauterine instillation. The PRP was activated and instilled within one hour of activation [8]. According to Dogra et al. [8], PRP preparations should contain platelet concentration exceeding 1 million/µL, providing an abundant source of growth factors [13]. To ensure quality, a hemocytometer (BOECO™ Neubauer Improved, Hamburg, Germany) was used to analyze two to three drops of the PRP product, confirming that platelet counts were 4–5 times higher in the serum [4, 5]. A complete blood count (CBC) was also performed to verify PRP concentration.
The final PRP preparation (1 mL) was instilled into the uterine cavity using an intrauterine insemination catheter (Gynetics, Gynétics Medical Products NV, Lommel, Belgium) under transabdominal ultrasound guidance and sterile conditions. All instillations were performed by a single operator.
ET in the frozen-thawed cycle followed standard protocols and lasted approximately 15–20 minutes. Participants were advised to empty their bladder before the procedure and were positioned in the lithotomy position under sterile conditions. A physician inserted a sterile speculum and an ET catheter. The embryo, either at the e blastocyst stage (D5) or cleavage stage (D3), was transferred into the uterine cavity under transabdominal ultrasound guidance, approximately 1–2 centimeters below the uterine fundus. After the procedure, participants rested in bed for 30 minutes before resuming normal activities.
Based on the RCT by Nazari et al. [15], average endometrial thickness
was compared among three groups: the control group, the single-intervention
group, and the double-intervention group, with mean values of 5.76
Baseline characteristics, including demographic data, reproductive history, and
underlying conditions, were analyzed using the Student’s t-test.
Continuous data was reported as mean
A total of 30 participants with thin endometrium were enrolled after meeting the
eligibility criteria. 3 individuals were withdrawn due to endometrial thickness
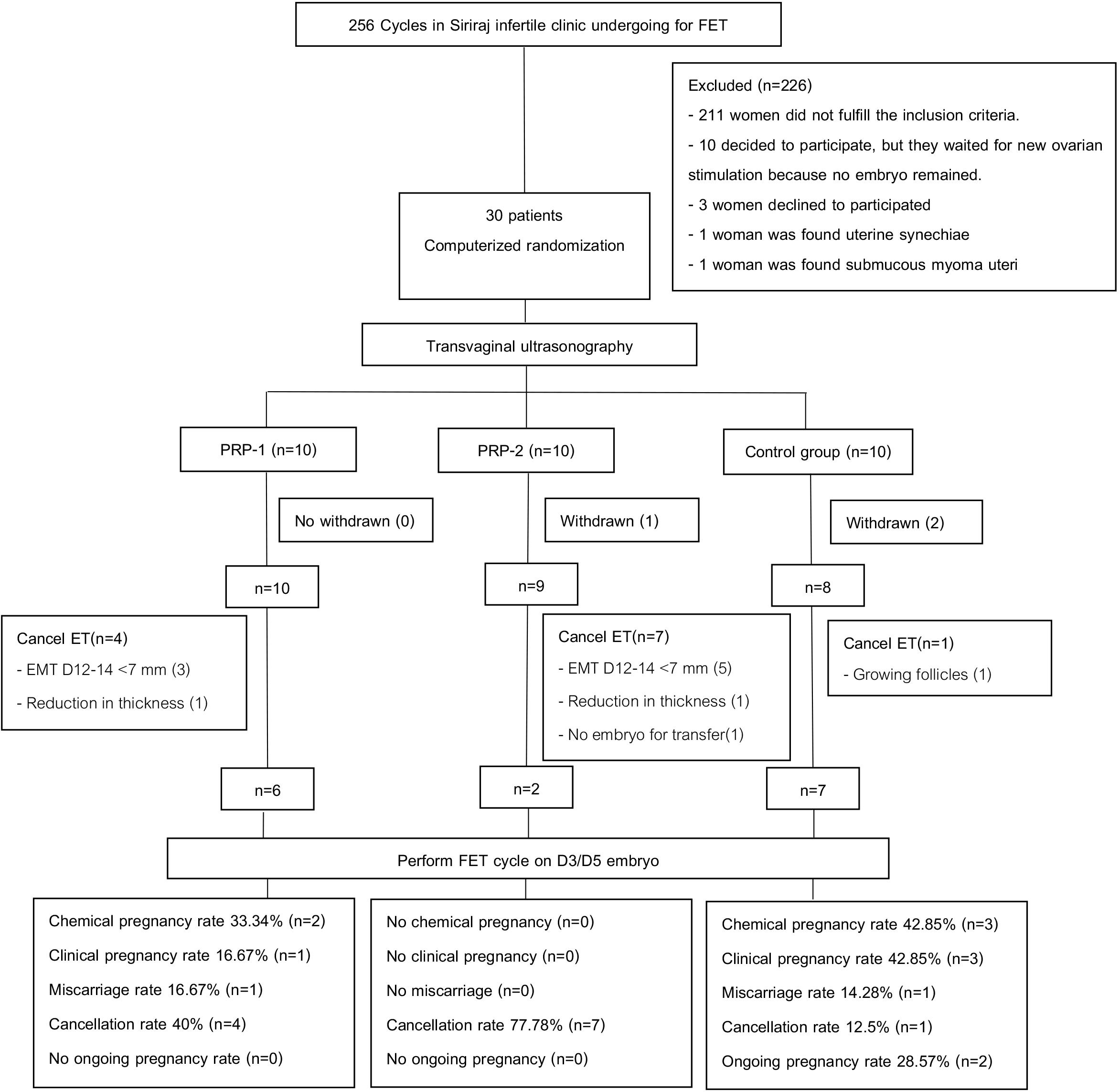 Fig. 1.
Fig. 1.
Study flowchart. FET, frozen embryo transfer; PRP, platelet-rich plasma; ET, embryo transfer; EMT, endometrial thickness; D, day of menstruation cycle.
| Patient characteristics | PRP-1 group | PRP-2 group | Control group | All group | ||
| (n = 10) | (n = 9) | (n = 8) | (n = 27) | |||
| Age (yr.)* | 43.22 |
36.98 |
41.71 |
40.70 | ||
| AMH (ng/mL)# | 0.68 (0.08, 1.71) | 2.02 (1.37, 3.69) | 1.32 (0.37, 2.59) | 1.32 (0.60, 2.59) | ||
| BMI* | 22.35 |
23.98 |
22.49 |
22.95 | ||
| P# | 0 | 0 | 0 | 0 | ||
| A# | 1 (0.00, 2.00) | 1 (0.50, 2.00) | 0.5 (0.00, 1.75) | 1 (0.00, 2.00) | ||
| Infertile period (mo.)# | 49 (28.50, 81.50) | 26 (15.25, 45.50) | 31 (12.25, 47.00) | 36 (18.00, 59.00) | ||
| Previous FET# | 0 (0.00, 2.25) | 0 (0.00, 2.00) | 2 (0.00, 3.75) | 0 (0.00, 3.00) | ||
| Previous cancellation (times)# | 2 (1.00, 2.25) | 1 (1.00, 2.00) | 1 (1.00, 2.00) | 1 (1.00, 2.00) | ||
| Previous uterine curettage# | 0 (0.00, 2.00) | 1 (0.00, 1.50) | 0 (0.00, 0.75) | 0 (0.00, 1.00) | ||
| Number of embryos# | 1 (0.00, 2.00) | 0 (0.00, 0.50) | 1 (1.00, 1.75) | 1 (0.00, 1.00) | ||
| Serum platelet (platelets /µL)* | 307,500.00 |
337,111.00 |
- | 321,526.00 | ||
| PRP platelet (Million) | ||||||
| D8# | 5.80 (5.00, 6.20) | 5.40 (5.20, 6.40) | - | 5.80 (5.00, 6.20) | ||
| D10# | - | 3.17 (1.63, 5.39) | - | |||
| Embryo morphology (n) | ||||||
| D5 | ||||||
| Good quality | 1 | 1 | 1 | |||
| Fair quality | 2 | 1 | 5 | |||
| Poor quality | 1 | 0 | 0 | |||
| D3 | ||||||
| Good quality | 1 | 0 | 0 | |||
| Fair quality | 0 | 0 | 1 | |||
| Poor quality | 1 | 0 | 0 | |||
| Infertility factors, n (%) | ||||||
| Male | 3 (30.00) | 1 (11.11) | 4 (50.00) | |||
| Female | ||||||
| Uterine | ||||||
| Myoma uteri | 2 (20.00) | 4 (44.44) | 3 (37.50) | |||
| Adenomyosis | 0 | 1 (11.11) | 0 | |||
| Non-uterine | 8 (80.00) | 5 (55.60) | 6 (75.00) | |||
| RIF | 2 (20.00) | 4 (44.44) | 5 (62.50) | |||
| RPL | 4 (40.00) | 2 (22.22) | 2 (25.00) | |||
| APS | 0 | 1 (11.11) | 1 (12.50) | |||
| Unexplained infertility | 0 | 2 (22.22) | 1 (12.50) | |||
Abbreviations: AMH, antimullerian hormone; BMI, body mass index; P, parity; A, abortion; FET, frozen-thawed embryo transfer; PRP, platelet-rich plasma; D, day of menstruation cycle; RIF, recurrent implantation failure; RPL, recurrent pregnancy loss; APS, antiphospholipid syndrome; yr., year; mo., month.
Data presented as Mean
*Mean
Baseline platelet concentration in the PRP-1 and PRP-2 groups were 0.30
A total of 28 PRP attempts were performed, with endometrial thickness and ART outcomes evaluated. All participants undergoing FET cycles followed the same hormone replacement therapy (HRT) protocol. The median number of embryos transferred was 1 (range: 0, 1), with 66.67% transferred on D5 (10/15), and 33.33% transferred on D3 (5/15). According to the Istanbul Consensus 2011 (Supplementary Material), and 26.67% were classified as good-quality embryos (2 embryos in PRP-1, 1 embryo in PRP-2, and 1 embryo in Control), 53.55% as fair quality embryos (3 embryos in PRP-1, 1 embryo in PRP-2, and 4 embryos in Control), and 20% as poor quality embryos (1 embryo in PRP-1 and 2 embryos in Control).
To evaluate whether PRP improved reproductive outcomes in patients with thin
endometrium, we analyzed changes in endometrial thickness and pregnancy outcomes.
The greatest increase in endometrial thickness was observed in the PRP-1 group
(1.52
| Outcomes | PRP-1 group (n = 10) | PRP-2 group (n = 9) | Control group (n = 8) | p-value | |
| Preparation duration (days) | 18.80 |
15.89 |
18.13 |
0.278 | |
| Endometrial thickness (mm) | |||||
| D3 | 3.85 |
4.03 |
4.31 |
0.726 | |
| D8 | 5.04 |
5.76 |
6.18 |
0.027† | |
| D12 | 6.56 |
6.48 |
7.60 |
0.040† | |
| Endometrial thickness difference between D8 to D12 | 1.52 |
0.72 |
1.43 |
0.153 | |
Data presented as Mean
† Statistically significant.
Endometrial thickness shows significant difference among the groups on D8 and D12, p = 0.027 (Control vs. PRP-1 p = 0.028†) and p = 0.040, respectively (Control vs. PRP-2 p = 0.004†).
Secondary outcome analyses is demonstrated in Table 3. The chemical pregnancy rates were 33.34%, 0%, and 42.85% (p = 0.790) in the PRP-1, PRP-2, and control groups, respectively. Clinical pregnancy rates were 16.67%, 0% and 42.85% (p = 0.585), respectively; ongoing pregnancy rates were 0%, 0%, and 28.57% (p = 0.600), respectively; and the miscarriage rates were 16.67%, 0%, and 14.28% (p = 1.000), respectively. Notably, the cycle cancellation rate was significantly higher in the repeated PRP group (77.78%) than in the control group 12.5% (p = 0.015).
| Secondary outcomes | PRP-1 group (n = 6) | PRP-2 group (n = 2) | Control group (n = 7) | p-value |
| Chemical pregnancy, n (%) | 2 (33.34) | 0 | 3 (42.85) | 0.790 |
| Clinical pregnancy, n (%) | 1 (16.67) | 0 | 3 (42.85) | 0.585 |
| Ongoing pregnancy, n (%) | 0 | 0 | 2 (28.57) | 0.600 |
| Abortion rate, n (%) | 1 (16.67) | 0 | 1 (14.28) | 1.000 |
| Cancellation rate, n (%) | 4 (40.00) | 7 (77.78) | 1 (12.50) | 0.027† |
† Statistically significant.
Cancellation rate shows significant differences among the groups (p = 0.027).
Pairwise comparisons showed no significant difference between the Control vs. PRP-1 (p = 0.314), or between PRP-1 and PRP-2 (p = 0.170), but a significant difference was observed between the Control vs. PRP-2 (p = 0.015†).
Among the 19 women who underwent 28 PRP attempts, no serious adverse events such as pain, irritation, or infections related to the PRP procedure were reported (70.37%). This suggests that PRP instillation is well-tolerated and safe.
This study investigated the effects of intrauterine instillation of autologous PRP on endometrial thickness and pregnancy outcomes in infertile women undergoing FET cycles. Our findings indicate that a single PRP instillation resulted in higher endometrial thickness compared to the control group; however, this difference was not statistically significant. In contrast, repeated PRP instillations showed limited benefit in increasing endometrial thickness and were associated with a higher cycle cancellation rate.
The observed increase in endometrial thickness in the PRP-1 group aligns with
previous studies [16, 17, 18, 19], which suggest that PRP promotes angiogenesis and tissue
regeneration through growth factors such as VEGF, PDGF, and IGF-1 [4, 11, 12].
Similarly, a 2024 meta-analysis [20] and a recent 2025 Turkish study [21]
showed that PRP can increase endometrial thickness. However, the lack of
statistical significance in our study, compared to previous reports, may be
explained by the control group starting with a higher endometrial thickness after
5 days of standard HRT (D8; Control vs. PRP-1). Despite this, following the full
effect of PRP instillation, the PRP-1 group demonstrated a greater increase in
thickness compared to the control group (1.52
Table 2 shows that the difference in mean endometrial thickness among the three groups reached only marginal statistical significance. Although the 1.52 mm gain observed in the PRP-1 group did not translate into higher pregnancy or live-birth rates, it may still increase the chance of proceeding to ET in women with a history of repeated cycle cancellations.
Although the PRP-1 group exhibited improved endometrial thickness, no significant differences were observed among the groups in terms of clinical pregnancy rates, chemical pregnancy rates, ongoing pregnancy rates, or miscarriage rates. These results are consistent with previous studies. Allahveisi et al. (2020) [22] reported no significant differences between PRP and control groups in chemical pregnancy rates (28% vs. 36%) and clinical pregnancy rates (28% vs. 24%). Similarly, Aghajanzadeh et al. (2020) [9] found no significant differences in chemical pregnancy, clinical pregnancy, and ongoing pregnancy rates. One potential explanation for these findings is the baseline characteristics of our study population, which included a high proportion of patients with unfavorable prognostic factors, such as refractory thin endometrium and RIF. The absence of significant differences in pregnancy rates highlights the need for further investigation into the effects of PRP on additional implantation-related factors and pregnancy outcomes, including the potential impact on embryonic chromosomal abnormalities. Notably, this study did not include embryos screened by Preimplantation Genetic Testing for Aneuploidy (PGT-A).
In contrast, the PRP-2 group did not show improvements in endometrial thickness and had a significantly higher cycle cancellation rate, which differs from the findings by Nazari et al. (2019) [15]. Although the exact causal relationship of repeated PRP treatment is not fully understood, it may be influenced by various factors, including the accumulation of excessive endometrial fluid inside the uterine cavity following repeated PRP administration [23, 24]. This may lead to endometrial dysfunction, potentially disrupting the endometrial microenvironment, similar to conditions like hydrosalpinx or uterine isthmocele. Excess intrauterine fluid may also increase uterine peristalsis, potentially leading to embryo expulsion [25]. In future research, we recommend more precise diagnostic evaluations to detect intrauterine fluid or hydrosalpinx fluid (e.g. 3D-ultrasonography, office hysteroscopy) in cases where PRP was instilled into the uterine cavity and the cycle was cancelled, in order to confirm this hypothesis.
Furthermore, the PRP-2 group exhibited a significantly higher cycle cancellation rate (77.78%) compared to the PRP-1 and control groups. The underlying mechanism for this increased cancellation rate remains unclear but may be associated with excessive exposure to PRP, growth factors, or cytokines beyond an optimal therapeutic range.
To our knowledge, this is the first RCT study to compare the effects of single PRP instillation, repeated PRP instillation, and standard hormone replacement therapy on endometrial thickness and ART outcomes. Additionally, this study examined both baseline serum platelet concentrations and platelet concentrations in PRP preparations to ensure that each sample contained more than 1 million platelets per preparation, to maximizing PRP quality [8]. Another key finding is that repeated PRP instillations do not appear to provide additional benefits for endometrial thickness and may, in fact, contribute to higher cycle cancellation rates. Therefore, a single PRP instillation should be considered as an alternative treatment option for patients with thin endometrium who fail to achieve the target thickness after standard hormonal treatment.
This study has some limitations. First, the inclusion of non-next generation sequencing (NGS) embryos may have influenced ART success rates, particularly given the average participant age of 40 years. However, pregnancy rates were not the primary focus of this study, and the absence of NGS did not impact the primary outcome of interest (endometrial thickness). Second, the study population included patients with inherently poor prognoses, such as those with refractory thin endometrium or RIF. While a single PRP instillation increased endometrial thickness, the difference was not statistically significant in this study. Third, our study excluded women with intrauterine adhesions, who may represent one of the targets that could benefit from PRP treatment. A recent study [26] and meta-analysis [27] have shown that PRP can increase other aspects of reproductive function, such as increase menstrual blood flow, improving menopausal hormonal profile, or increasing the Anti-Mullerian Hormone (AMH) level.
Finally, although the data were sufficient for analysis, the small sample size warrants cautious the interpretation of the results. Therefore, future RCT studies should include larger sample sizes to increase statistical power and aim to elucidate the comparative efficacy of single versus repeated PRP injections. Furthermore, future studies should include euploid embryos to better assess PRP’s effects on clinical pregnancy rates. Additionally, investigating endometrial receptivity through molecular markers (e.g., HOXA10, leukemia inhibitory factor [LIF]) assessing microbiome changes, before and after PRP administration, may provide valuable insights, particularly for patients with thin endometrium or RIF. Future research should also explore other reproductive aspects like anti-adhesive efficacy of PRP in postoperative intrauterine surgery, to decrease risk of adhesion recurrence or prevent adhesion formation, which represents an important area for further research.
The study found that a single intrauterine PRP instillation prior to a FET cycle improved endometrial thickness, although the difference was not statistically significant. However, repeated PRP instillations did not provide additional benefits in endometrial thickness or ART outcomes and were associated with a higher cycle cancellation rate. These findings suggest that a single PRP injection may be sufficient to treat and improve thin endometrium in infertile women, potentially eliminating the need for repeated or multiple injections. Additionally, PRP instillation is a safe and straightforward method for enhancing endometrial thickness, but it does not appear to significantly improve ART outcomes. Further research is warranted to explore the long-term effects of PRP on pregnancy outcomes and to refine its clinical application in assisted reproductive technology.
All data is available upon request as a supplementary file. Please contact the corresponding authors for further information.
SPO, NP and SPE designed the project. SPO and NP performed the research and wrote the manuscript. SPO, NP, PL, SPE, IT, JP, PH and PT collected the data. SPO and NP analyzed the data. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
According to the guidelines of the Declaration of Helsinki, this study was approved by the Siriraj Institutional Review Board (Protocol No. 853/2566, IRB4; (COA No. Si 987/2023). The study has been registered on https://clinicaltrials.gov/ registration number: NCT06234540. All participants provided written informed consent.
We extend our gratitude to all participants and to the staff of the Siriraj Infertility Clinic. The authors would like to thank Dr. Saowalak Hunnangkul from Siriraj Research Data Management Unit (SI-RDMU) for guidance, support and assistance with computerized statistical analysis.
Faculty of Medicine, Siriraj Hospital, Mahidol University (R016233020).
The authors declare no conflicts of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG39260.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.