








 , Jalal Asadi 2, Zeinab Hemmati 3, Lotfolah Saed 4, Elham Nouri 2, Yousef Moradi 5,*
, Jalal Asadi 2, Zeinab Hemmati 3, Lotfolah Saed 4, Elham Nouri 2, Yousef Moradi 5,*
1 Student Research Committee, Kurdistan University of Medical Sciences, 66377-31996 Sanandaj, Iran
2 Department of Epidemiology and Biostatistics, Faculty of Medicine, Kurdistan University of Medical Sciences, 66377-31996 Sanandaj, Iran
3 Department of Obstetrics and Gynecology, School of Medicine, Kurdistan University of Medical Sciences, 66377-31996 Sanandaj, Iran
4 Department of Endocrinology, Faculty of Medicine, Kurdistan University of Medical Sciences, 66377-31996 Sanandaj, Iran
5 Social Determinants of the Health Research Center, Research Institute for Health Development, Kurdistan University of Medical Sciences, 66377-31996 Sanandaj, Iran
Abstract
Adequate thyroid hormone production is critical for fertility and the successful maintenance of pregnancy. Thyroid autoimmunity (TAI), characterized by the presence of thyroid peroxidase antibodies (TPOAb) and anti-thyroglobulin antibodies (TgAb), is the most common cause of thyroid dysfunction in women of reproductive age. The association between TAI and adverse reproductive outcomes, including infertility and pregnancy complications, has garnered significant attention, particularly in the context of assisted reproductive technology (ART).
This study is a systematic review and meta-analysis designed to examine the relationship between TAI and outcomes of ART. A comprehensive literature search was conducted in PubMed, Scopus, and Web of Science databases to identify relevant studies published up to May 1, 2022. In addition, articles published between May 2022 and May 2025 were included, along with earlier studies that were part of previous meta-analyses or provided novel and relevant findings. Studies were eligible for inclusion if they compared ART outcomes between women with TAI (defined by the presence of TPOAb and/or TgAb) and euthyroid women without thyroid autoantibodies. Evaluated outcomes included clinical pregnancy, miscarriage, live birth, implantation, and fertilization rates (FR). Statistical analysis was conducted using STATA version 18, with pooled odds ratios (ORs) and 95% confidence intervals (CIs), calculated using a random-effects model. Study heterogeneity was assessed using the I2 statistic.
A total of 30 studies were included in the meta-analysis to assess the association between TAI and ART outcomes. TAI was not significantly associated with clinical pregnancy rate (CPR) (OR: 0.91; 95% CI: 0.76–1.08), miscarriage rate (MR) (OR: 1.13; 95% CI: 0.93–1.38), or live birth rate (LBR) (OR: 0.97; 95% CI: 0.78–1.22). However, significant negative associations were found between TAI and both implantation rate (IR) (OR: 0.82; 95% CI: 0.72–0.93) and FR (OR: 0.87; 95% CI: 0.83–0.90). Subgroup analysis revealed a more pronounced adverse effect of TAI on CPR among women undergoing in vitro fertilization (IVF) compared to intracytoplasmic sperm injection (ICSI). These findings suggest TAI may impair specific ART outcomes, particularly embryo implantation and fertilization.
Autoimmune thyroid disease may affect certain ART outcomes, such as a reducing FR; however, no significant difference was observed in LBRs, suggesting that it may not significantly impact the overall success of ART in terms of live births. Monitoring thyroid function in women with TAI undergoing ART is recommended by multiple endocrinology society guidelines and may offer significant clinical beneficial. This includes assessing thyroid-stimulating hormone (TSH) levels at the time of the second positive human chorionic gonadotropin (hCG) result, which confirms pregnancy.
The study has been registered on https://www.crd.york.ac.uk/prospero/ (registration number: CRD42023488835; registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42023488835).
Keywords
- autoimmune disease
- assisted reproductive technology
- pregnancy outcome
- thyroid autoimmunity
- evidence-based medicine
Thyroid dysfunction disrupts the menstrual cycle, impairs women’s fertility, and affects pregnancy outcomes, and is classified as the second most common endocrine disorder in women of reproductive age [1]. Thyroid-stimulating hormone (TSH) has been recognized as an important factor in reproductive health conditions for several decades. The risk of infertility in patients with thyroid disorders increases due to its association with elevated prolactin levels. Therefore, primary hypothyroidism is a risk factor for reproductive failure, with the prevalence of autoimmune thyroid disorders in women of reproductive age ranging from 5% to 20% [2].
These adverse pregnancy outcomes can encompass a wide range of effects, including increased incidences of infertility, miscarriage, and unfavorable obstetric and fetal complications [3]. Thyroid autoimmunity (TAI) is the primary cause of primary hypothyroidism. When the thyroid tissue is damaged by autoantibodies, it may eventually be destroyed, resulting in the loss of normal function [4]. TAI is the most common autoimmune condition and the leading cause of thyroid dysfunction in women of reproductive age [5].
Autoimmune thyroid disorders are characterized by the presence of
anti-thyroglobulin antibodies (TgAb) and anti-thyroid peroxidase antibodies
(TPOAb). TPOAb are not used as a screening test for hypothyroidism, as TSH
remains the primary marker of thyroid function. However, the presence of TPOAb
can indicate an increased risk of developing hypothyroidism during early
pregnancy and postpartum thyroid dysfunction in women at higher risk for thyroid
disorders [6]. TAI can lead to immune dysfunction and suppression of immune
tolerance at the systemic maternal-fetal interface. Additionally, inflammatory
cytokines such as interleukin (IL)-2, IL-17, and interferon-gamma (IFN-
According to a report by the World Health Organization, infertility affects 15% of couples of reproductive age worldwide, driving the increased use and expansion of assisted reproductive methods globally [10]. The increase in infertility rates (8.5%) in developed countries is partly attributed to the growing demand for ART [11].
Most infertile couples undergo ART, including in vitro fertilization (IVF) and intracytoplasmic sperm injection (ICSI). IVF and embryo transfer (IVF-ET) is one of the most commonly used assisted reproductive techniques and has shown increasing success rates since it was first introduced in 1978 [12]. IVF treatment has helped couples struggling with infertility to give birth to over 8 million babies worldwide. Despite improvements in stimulation protocols and laboratory techniques, the live birth rate (LBR) per cycle has remained between 19% and 22%. This highlights the continued influence of various factors that may affect treatment success and the overall ART process [12].
The impact of TAI on the outcomes of ART has been extensively studied; however, significant heterogeneity exists among studies due to variations in study design, causes of infertility, ovarian stimulation protocols, definitions of euthyroidism, fertility methods (e.g., IVF, ICSI, or intrauterine insemination [IUI]), and outcome measures [13].
Autoimmune disorders may play a role in reproductive failures, as studies have shown that both in spontaneous pregnancies and those achieved through ART, euthyroid women with TAI and women with thyroid dysfunction (subclinical) experience miscarriage in 20 to 30 percent of cases [14, 15, 16]. TAI is more prevalent in women of childbearing age and is independently associated with fertility and pregnancy complications, both in cases of spontaneous pregnancies or after treatment with ART [15]. Several studies have reported unfavorable outcomes in the treatment of IVF/ICSI among TAI-positive women, such as higher miscarriage rates (MRs), lower embryo quality, and reduced chances of live birth, even in the presence of normal thyroid function [17, 18, 19]. However, other studies have found no significant association between TAI and pregnancy outcomes [20, 21, 22].
This systematic review and meta-analysis evaluated the association between TAI and ART outcomes. The protocol was registered in PROSPERO (CRD42023488835) and adhered to PRISMA (The Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines for reporting systematic reviews and meta-analyses.
Studies were included if they involved women undergoing ART procedures, such as IVF, ICSI, or IUI, with clearly defined TAI status based on the presence of TPOAb and/or TgAb. The exposure group consisted of women with TAI (TPOAb and/or TgAb positive), while the comparison group included TAI-negative women (TPOAb and TgAb negative). Eligible studies were required to report at least one of the following outcomes: LBR, fertilization rate (FR), implantation rate (IR), clinical pregnancy rate (CPR), or MR. Only prospective or retrospective cohort and case-control studies reporting odds ratios (ORs) with 95% CIs were included. Studies were excluded if they were case series, reviews, editorials, or lacked sufficient data for quantitative analysis (Table 1).
| Category | Inclusion criteria | Exclusion criteria |
| Population | Women undergoing ART (IVF, ICSI, or IUI). | Studies without ART participants or non-human subjects. |
| Exposure | TAI status determined by TPOAb or TgAb positivity. | Studies not assessing TAI or using unclear or incomplete TAI criteria. |
| Comparison | Women without TAI (TPOAb and TgAb negative). | Studies lacking a comparison group of TAI-negative women. |
| Outcomes | LBR, FR, IR, CPR, MR as defined by ART clinical standards. | Studies not reporting at least one predefined outcome. |
| Study design | Cohort or case-control studies (prospective or retrospective) reporting [OR or risk ratio (RR) with 95% CI]. | Case series, reviews, editorials, or studies with incomplete data. |
| Language | Articles published in English. | Studies published in languages other than English. |
| Timeframe | Studies published from May 2022 to May 2025 onward were included in this meta-analysis. Studies published before May 2022 were also considered if they had been included in prior meta-analyses or if they provided new, relevant data for the current analysis. | - |
| Search terms | Thyroid autoantigen-related terms: “thyroglobulin antibodies”, “thyroid gland”, “graves’ disease”, “graves hyperthyroidism”, “thyroid peroxidase antibody”, “thyroid autoantibody”, “thyroid autoimmunity”, “autoantibodies”, “autoimmune thyroiditis”, “thyroiditis”, “anti-thyroglobulin”, “antithyroglobulin”, “antithyroglobulin antibody”, “hyperthyroidism”, “thyroid stimulating hormone”. | - |
| ART-related terms: “Intracytoplasmic sperm injection”, “in vitro fertilization”, “assisted reproduction”, “assisted conception”, “assisted reproductive technology”, “ICSI”, “IVF”, “sperm injections”, “ART”, “intracytoplasmic”, “assisted reproductive techniques”. | ||
| Outcome-related terms: “fertility”, “pregnancy”, “miscarriage”, “delivery”, “live birth rate”, “implantation rate”, “clinical pregnancy rate”, “fertilization rate”. | ||
| Databases | PubMed (Medline) | - |
| Scopus | ||
| Web of Science |
ART, assisted reproductive technology; IVF, in vitro fertilization; ICSI, intracytoplasmic sperm injection; IUI, intrauterine insemination; TPOAb, thyroid peroxidase antibodies; TAI, thyroid autoimmunity; TgAb, anti-thyroglobulin antibodies; LBR, live birth rate; FR, fertilization rate; IR, implantation rate; CPR, clinical pregnancy rate; MR, miscarriage rate; OR, odds ratio; CI, confidence interval.
The first stage of this study involved implementing a comprehensive search strategy using relevant keywords aligned with the research question. A well-defined search protocol was designed and executed across three major international databases: PubMed (Medline), Scopus, and Web of Science (Table 1). The search targeted studies that explored the relationship between TAI and ART outcomes, including in IVF, ICSI, IUI, or ovulation induction.
The search was limited to studies published in English, and only prospective or retrospective cohort and case-control studies were eligible for inclusion. Eligible studies were those comparing IVF/ICSI outcomes between women positive for TAI (TAI-positive) and those negative for thyroid autoantibodies (TAI-negative). The titles and abstracts of articles identified in the initial search were reviewed by two independent reviewers (JA and HG) to exclude studies that did not meet the predetermined eligibility criteria or address the research question. Full-text articles of the remaining studies were then assessed for relevance and eligibility. In addition to the database search, reference lists of the included studies were systematically reviewed to identify other potentially eligible studies for inclusion in the meta-analysis. This current analysis builds upon the findings of the previous meta-analysis by Busnelli et al. [23], which also explored the relationship between TAI and ART outcomes. This meta-analysis included studies published from May 2022 to May 2025. Studies published before May 2022 were also considered if they had been included in previous meta-analyses or provided new, relevant data for the current analysis.
Exclusion criteria from the study included: duplicate studies, studies published in languages other than English, studies lacking a control or non-patient group, studies involving concomitant drug treatments that could affect the outcomes, studies with incomplete data, and reviews or meta-analyses.
The methodological quality of the included studies was independently assessed by two reviewers (JA and HG) using the Newcastle-Ottawa Scale (NOS) for observational studies. The NOS evaluates study quality based on three domains: Selection (maximum 4 stars), Comparability (maximum 2 stars), and Outcome (maximum 3 stars). Each study could receive a maximum of 9 stars. Studies scoring 6 or more stars were considered to be of moderate to high quality. Disagreements between reviewers were resolved through discussion or consultation with a third reviewer [24].
All statistical analyses were performed using Stata version 18 (StataCorp LLC, College Station, TX, USA). Dichotomous outcomes (including CPR, MR, LBR, IR, and FR) were analyzed using ORs with corresponding 95% CIs. Meta-analyses were conducted using the DerSimonian and Laird random-effects model to account for between-study variability. Heterogeneity among studies was assessed using the Cochran’s Q test and quantified with the I2 statistic. Thresholds of 25%, 50%, and 75% were used to indicate low, moderate, and high heterogeneity, respectively. Subgroup analyses were conducted to evaluate the influence of different ART methods (IVF vs. ICSI) on outcomes. Q statistics were used to assess differences between subgroups. Publication bias was statistically tested using Egger’s regression test.
Fig. 1 illustrates the process of study identification and selection. The search yielded a total of 338 studies from the PubMed (91 articles), Scopus (187 articles), and Web of Science (60 articles) databases, of which 98 duplicates were subsequently removed. After removing duplicates using EndNote software, 240 articles were screened by the authors. Of these, 210 were excluded based on their titles and abstracts for not meeting the predefined selection criteria. Initially, 30 studies were deemed eligible for inclusion. However, upon full-text thorough review, 7 studies were excluded because they were systematic reviews or meta-analyses, and 5 studies were excluded for being published prior to the most recent update (May 2022). Additionally, 7 articles were excluded due to differing study types, and 5 studies were excluded because their objectives did not align with the focus of our study. Studies involving treatments or interventions that did not meet the predefined criteria were also excluded. Consequently, 8 studies were selected for inclusion in the analysis. When combined with 22 articles from the previous update, a total of 30 studies were reviewed to extract relevant outcomes (Fig. 1 and Table 2, Ref. [18, 20, 22, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51]).
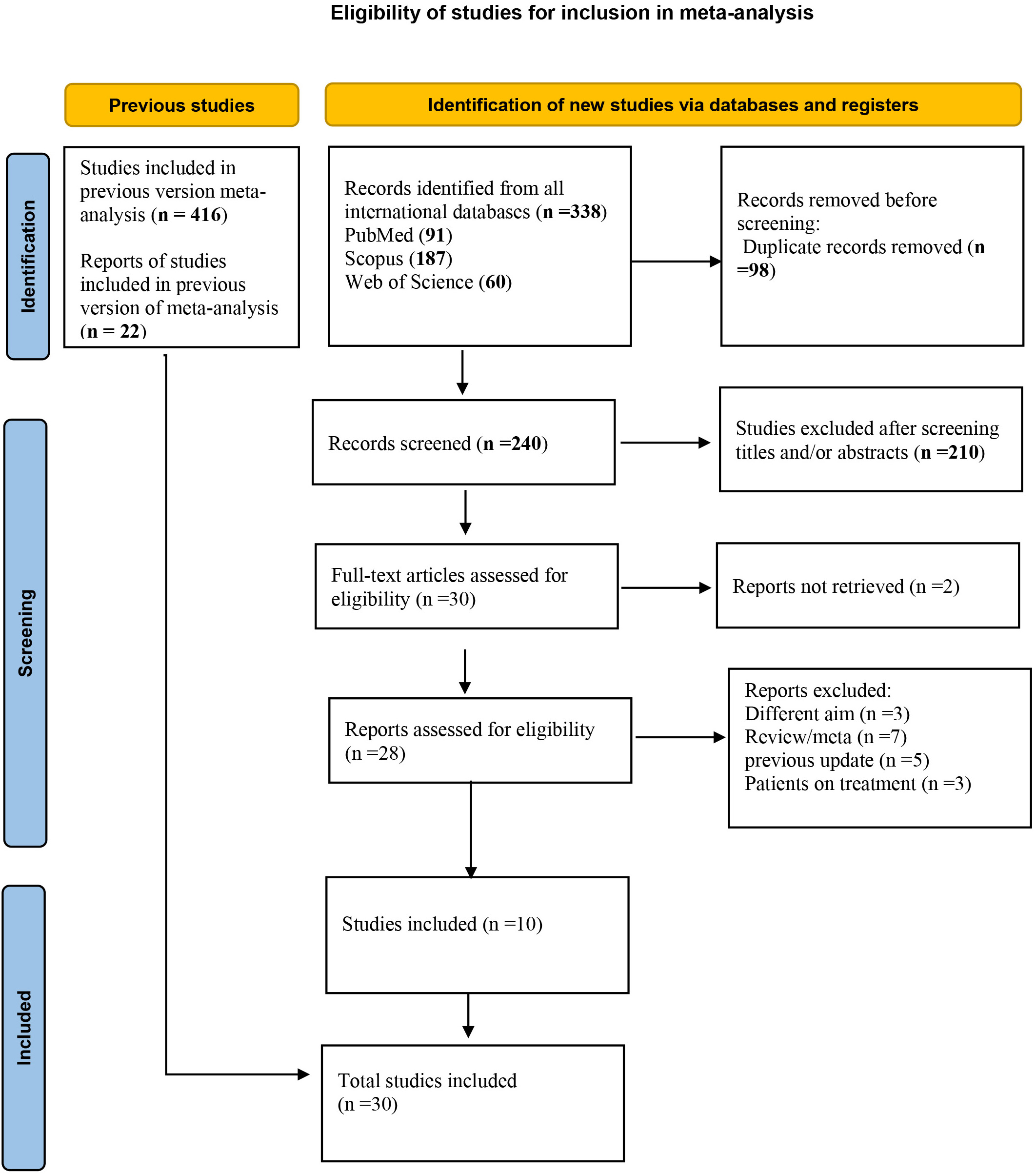 Fig. 1.
Fig. 1.
Eligibility of studies for inclusion in meta-analysis.
| Authors | Year | Country | Design | Total sample size | Number of TAI+ | Number of TAI– | IVF & ICSI | TSH range in cases | Thyroid function tests | Outcome | NOS score |
| Zhang Y et al. [25] | 2023 | China | Prospective cohort study | 464 | 225 | 239 | IVF or ICSI | low-normal group, |
D14 TSH | CPR, MR, LBR | 9 |
| high-normal group, 2.5–4.2 | |||||||||||
| 374 | 135 | 239 | low-normal group, |
TSH levels | CPR, MR, LBR | 7 | |||||
| high group, | |||||||||||
| Herman T et al. [26] | 2023 | Hungary | Prospective cohort study | 231 | 161 | 70 | IVF | TSH had to be below 2.5 mIU/L | TPOAb or TGAb | CPR | 7 |
| Liu Y et al. [27] | 2023 | China | Prospective cohort study | 1279 | 518 | 779 | IVF or ICSI | 2.15 mIU/L | NR | CPR, MR | 5 |
| Liu Y et al. [28] | 2022 | China | Prospective cohort study | 206 | 103 | 103 | IVF or ICSI | NR | NR | CPR, FR | 7 |
| Yang X et al. [29] | 2023 | China | Retrospective cohort study | 2987 | 533 | 2454 | IVF or ICSI | NR | TPOAb; TgAb | CPR, MR, LBR, FR | 7 |
| Medenica S et al. [30] | 2023 | Serbia | Prospective cohort study | 52 | 26 | 26 | IVF or ICSI | 0.40–4.00 mIU/mL | TPOAb; TgAb | CPR | 9 |
| Cevher Akdulum MF et al. [31] | 2022 | Turkey | Prospective cohort study | 918 | 363 | 555 | IVF or ICSI | 2.35 |
TPOAb; TgAb | CPR, MR | 9 |
| Moon KY et al. [32] | 2023 | Korea | Prospective cohort study | 215 | 29 | 188 | IVF | TSH 0.27–4.20 Subclinical hypothyroidism was defined as serum TSH |
TPOAb; TgAb | CPR, MR | 9 |
| Zhang R et al. [33] | 2022 | China | Cohort study | 180 | 120 | 60 | IVF or ICSI | TSH |
TPOAb; TgAb | CPR, LBR, IR | 7 |
| Zhong YP et al. [18] | 2012 | China | Case-control | 766 | 90 | 676 | IVF or ICSI | 2.35 |
NR | CPR, IR, FR | 5 |
| Karacan M et al. [34] | 2013 | Turkey | Prospective cohort study | 253 | 34 | 219 | ICSI | NR | NR | CPR, MR, IR | 7 |
| Litwicka K et al. [35] | 2015 | Italy | Prospective study | 164 | 30 | 134 | ICSI | TSH 0.27–4.20 | NR | CPR, MR, LBR | 7 |
| Lukaszuk K et al. [36] | 2015 | Poland | Retrospective cohort study | 665 | 114 | 551 | ICSI | NR | TPOAb; TgAb | CPR, LBR, FR | 6 |
| Gungor and Dokuzeylul Gungor [37] | 2021 | Turkey | Retrospective cohort study | 85 | 39 | 46 | ICSI | TSH |
NR | CPR, MR, LBR, FR | 6 |
| Liu Y et al. [38] | 2020 | China | Case-control study | 112 | 49 | 63 | IVF or ICSI | NR | NR | CPR, MR, LBR, IR | 6 |
| Chen X et al. [39] | 2017 | China | Prospective cohort study | 1293 | 449 | 844 | IVF or ICSI | NR | NR | CPR, MR, LBR, IR | 7 |
| Devi AB et al. [40] | 2019 | India | Prospective cohort study | 81 | 17 | 64 | IVF | 1.89–1.18 mIU/L | TSH- fT4; TPOAb; TgAb | CPR, IR, FR, IR | 6 |
| Kutteh WH et al. [41] | 1999 | USA | Retrospective cohort study | 873 | 143 | 730 | ICSI | NR | NR | CPR, MR, FR | 7 |
| Huang N et al. [42] | 2021 | China | Retrospective cohort study | 1556 | 778 | 778 | IVF or ICSI | NR | NR | CPR, LBR | 5 |
| Muller AF et al. [43] | 1999 | Netherlands | Nested case control study | 173 | 25 | 143 | IVF | NR | NR | CPR, MR | 7 |
| Tan S et al. [44] | 2014 | Germany | Retrospective cohort study | 835 | 110 | 725 | ICSI | 1.8–0.6 mIU/L | TSH; TPOAb; TgAb | CPR, MR | 7 |
| Sakar MN et al. [45] | 2016 | Turkey | Prospective case control study | 152 | 31 | 121 | IVF | 1.89–1.18 mIU/L | NR | CPR, MR | 7 |
| Poppe K et al. [46] | 2003 | Belgium | Prospective cohort study | 234 | 32 | 202 | IVF or ICSI | NR | NR | CPR, MR, LBR | 6 |
| Negro R et al. [47] | 2005 | Italy | Prospective cohort study | 662 | 86 | 576 | IVF or ICSI | NR | NR | CPR, MR | 5 |
| Negro R et al. [48] | 2007 | Italy | Prospective cohort study | 416 | 42 | 374 | IVF or ICSI | 0.5–2.5 mIU/L | TSH; TPOAb | CPR, MR, LBR | 7 |
| Mintziori G et al. [49] | 2014 | Greece | Retrospective cohort study | 85 | 17 | 68 | IVF | 1.8–0.6 mIU/L | NR | CPR, LBR | 6 |
| Chai J et al. [22] | 2014 | China | Retrospective cohort study | 508 | 89 | 419 | IVF or ICSI | NR | NR | CPR, MR, LBR | 5 |
| Tokgoz VY et al. [50] | 2020 | Turkey | Retrospective cohort study | 315 | 65 | 250 | ICSI | NR | NR | CPR, MR | 5 |
| Ke H et al. [20] | 2020 | Turkey | Case-control study | 4101 | 709 | 3392 | IVF or ICSI | 2.1–0.3 mIU/L | TSH; TPOAb; TgAb | CPR, MR, LBR, IR | 9 |
| Unuane D et al. [51] | 2017 | Belgium | Retrospective cohort study | 3143 | 187 | 2956 | IUI | 0.5–2.5 mIU/L | NR | CPR, MR, LBR | 7 |
NOS, Newcastle-Ottawa Scale; NR, not reported; TSH, thyroid-stimulating hormone; TAI+, TAI-positive; TAI–, TAI-negative; RF, reference range.
The NOS scores for the 30 studies ranged from 4 to 9, with most studies scoring 5–7, indicating moderate to good quality. Studies providing detailed TSH ranges and thyroid function tests (e.g., Zhang et al., 2023 [25]; Ke H et al., 2020 [20]) scored highest (8–9), whereas those with missing data or small sample sizes scored lower (4–6) (Fig. 2).
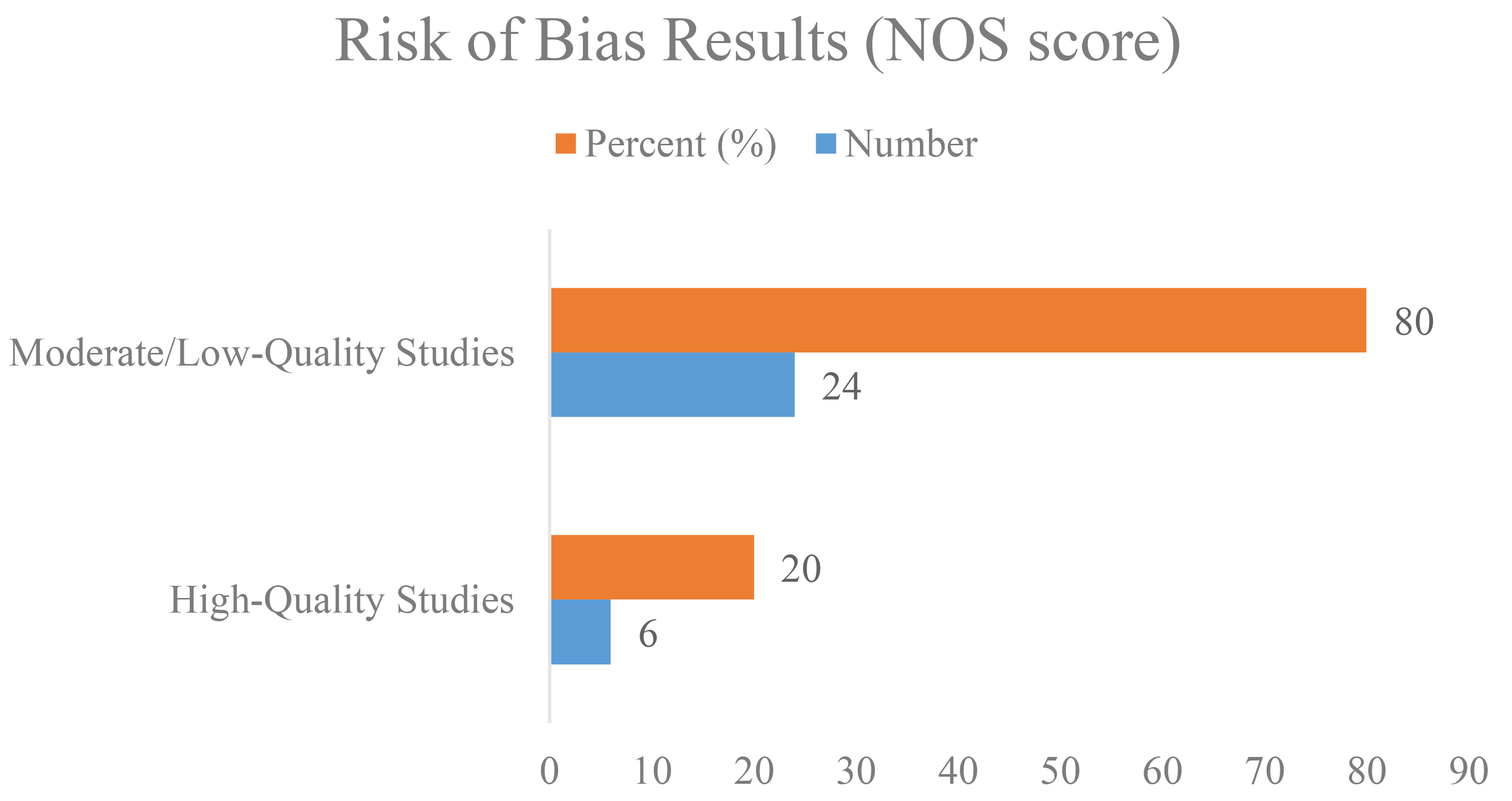 Fig. 2.
Fig. 2.
Risk of bias assessment of studies on TAI and ART outcomes using the NOS. ART, assisted reproductive technology; TAI, thyroid autoimmunity.
Of the studies included in the analysis, 29 studies compared CPR between patients with and without TAI, excluding two studies. The meta-analysis revealed no significant association between the presence of thyroid autoantibodies and clinical pregnancy. In fact, women without TAI showed CPRs similar to those with TAI. The pregnancy rate among women without autoimmune thyroid disease undergoing ART was only 9% lower than that of women with the condition. Both groups had nearly identical pregnancy rates following ART. The 95% CI: 0.76–1.08 includes 1, suggesting that the results were not statistically significant and that there is no meaningful difference between the two groups (random-effects model OR = 0.91) (Fig. 3). Egger’s test for publication bias in the meta-analysis of 29 studies comparing CPRs in women with and without TAI indicated no significant bias (b = 0.362, SE = 0.192, p = 0.623).
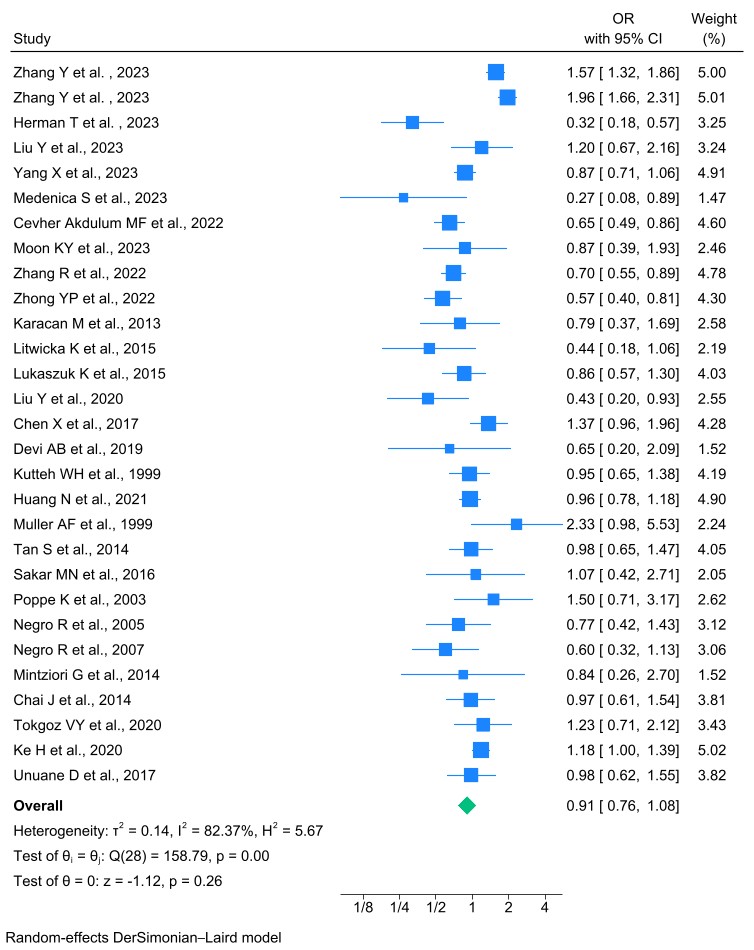 Fig. 3.
Fig. 3.
Forest plot of the association between thyroid autoantibody and CPRs. CPR, clinical pregnancy rate; OR, odds ratio; CI, confidence interval.
The meta-analysis of 22 studies (23 effect sizes) examining MR in women with TPOAb and/or TgAb undergoing IVF/ICSI revealed a 13% increase in MR among TAI-positive women compared to TAI-negative women. Although some individual studies reported significantly higher MR in the TAI-positive group, the overall meta-analysis did not show a statistically significant association between TAI and MRs (OR = 1.13, 95% CI: 0.93–1.38, p = 0.21). These findings suggest insufficient evidence to support a meaningful difference in MR between the two groups (Fig. 4). Additionally, Egger’s test for publication bias indicated no significant bias in this meta-analysis (b = 0.701, SE = 0.213, p = 0.290).
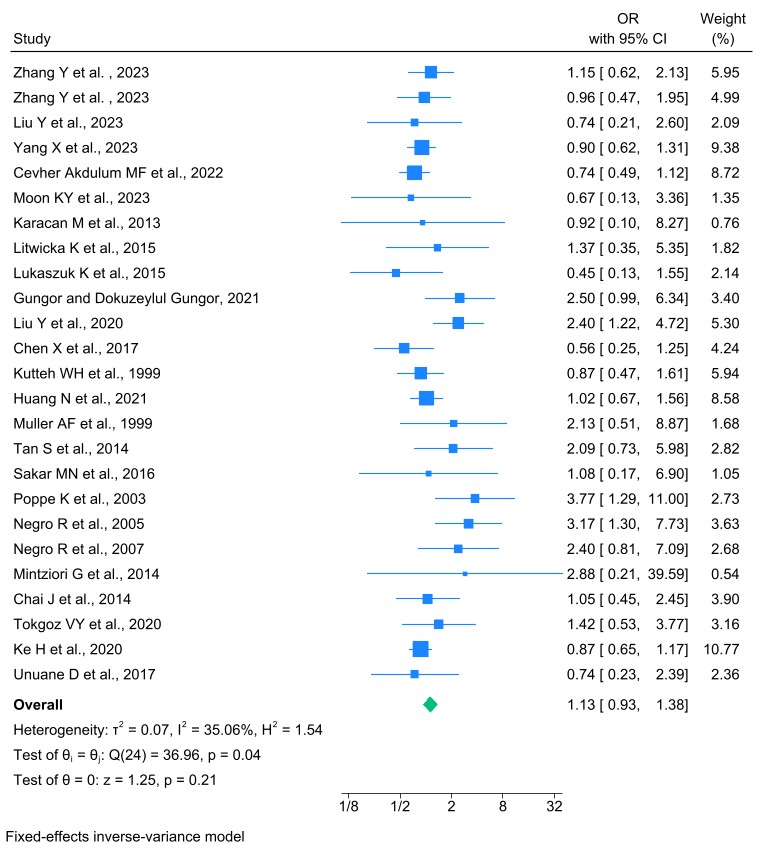 Fig. 4.
Fig. 4.
Forest plot of the association between thyroid autoantibody and MRs. MR, miscarriage rate.
14 studies investigated the LBR among women with TPOAb and/or TgAb undergoing IVF or ICSI. The difference in LBR between the healthy cohort and those with autoimmune thyroid disease was minimal, only just 2%, and not statistically significant. The meta-analysis revealed no significant association in LBRs between the TAI-positive (TAI+) and TAI-negative (TAI–) groups (p = 0.82). The random-effects model produced an OR of 0.97 (95% CI: 0.78–1.22), with a high degree of heterogeneity observed (I2 = 77.24%) (Fig. 5).
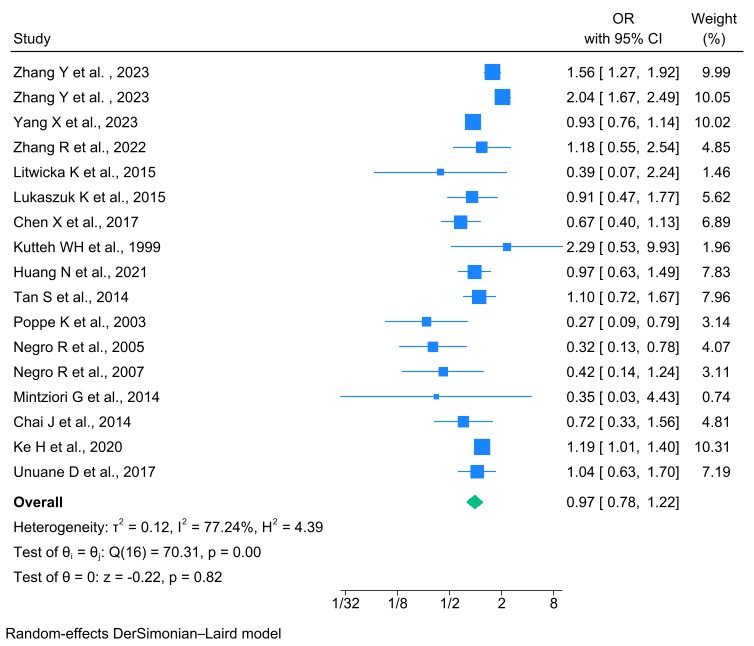 Fig. 5.
Fig. 5.
Forest plot of the association between thyroid autoantibody and LBRs. LBR, live birth rate.
The IR is defined as the percentage of transferred embryos that progress to at
least the stage of fetal heart activity, as confirmed by pregnancy ultrasound.
This meta-analysis included 8 studies involving women with TPOAbs or TgAbs
undergoing IVF/ICSI. The results indicated that women with TAI had a
significantly lower likelihood of achieving implantation compared to those
without TAI. An OR of 0.82, with a CI that does not include 1, suggests a
statistically significant protective effect in favor of the non-affected group.
This indicates that the presence of TAI is associated with a reduced likelihood
of implantation, and this difference was statistically significant (OR: 0.82,
95% CI: 0.72–0.93, I2 = 41.14%, p
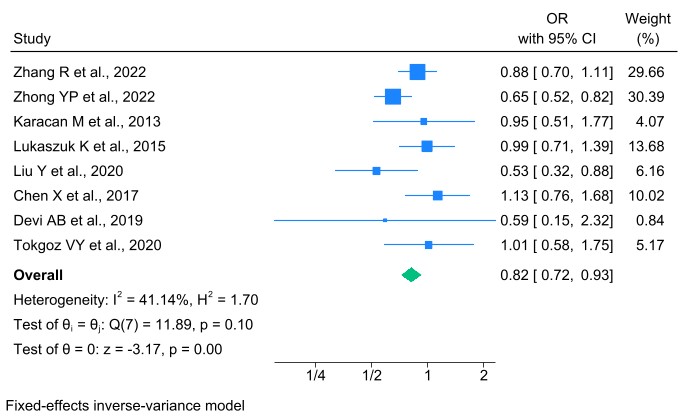 Fig. 6.
Fig. 6.
Forest plot of the association between thyroid autoantibody and IRs. IR, implantation rate.
Out of the 31 studies reviewed, 7 studies reported FR in women with TPOAb or
TgAb undergoing IVF/ICSI, as well as in TAI-negative controls. The results of the
meta-analysis indicated that the FR achieved through ART was significantly higher
in the TAI-negative group compared to the TAI-positive group. Specifically, the
OR was 0.87, indicating that the likelihood of fertilization in the TAI-positive
group was 13% lower than in the healthy (TAI-negative) group undergoing ART.
This suggests that TAI negatively impacts the chances of fertilization in women
undergoing ART. The difference was statistically significant (OR: 0.87, 95% CI:
0.83–0.90, I2 = 67.24%, p
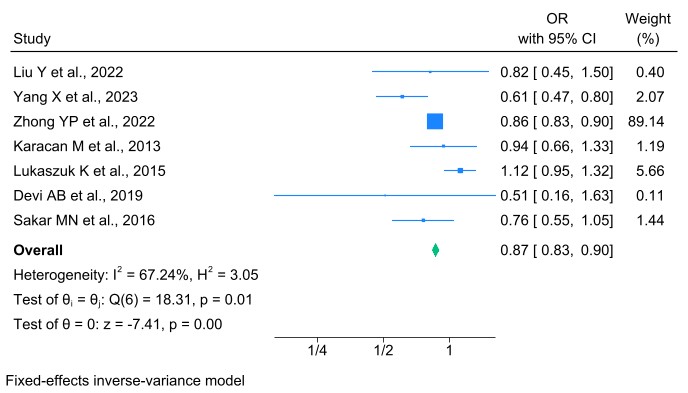 Fig. 7.
Fig. 7.
Forest plot of the association between thyroid autoantibody and FRs. FR, fertilization rate.
The meta-analysis revealed differences in CPRs among women with TAI undergoing different types of ART. Specifically, women undergoing IVF had a 28% lower CPR compared to healthy women undergoing IVF (OR: 0.72, 95% CI: 0.51–1.02). In contrast, among women undergoing ICSI, the CPR was only 8% lower compared to healthy women undergoing ICSI (OR: 0.92, 95% CI: 0.75–1.12). Importantly, the difference in CPRs between women with TAI undergoing IVF versus ICSI was statistically significant (Q = 8.91, p = 0.010). This indicates that the impact of TAI on CPRs varies depending on the type of ART, with a more pronounced reduction observed in IVF treatments (Table 3).
| Outcomes | Subgroups | OR (95% CI) | Heterogeneity assessment | ||||
| Between groups | Within groups | ||||||
| I2 % | Q | p-value | Q | p-value | |||
| CPR | IVF | 0.72 [0.51–1.02] | 67.71 | 15.48 | 0.01 | 8.91 | 0.010 |
| ICSI | 0.92 [0.75–1.12] | 0.00 | 4.16 | 0.53 | |||
| IVF & ICSI | 1.12 [1.05–1.20] | 88.47 | 130.07 | 0.00 | |||
| MR | IVF | 1.35 [0.56–3.23] | 0.00 | 1.49 | 0.68 | 1.09 | 0.580 |
| ICSI | 1.21 [0.83–1.76] | 15.74 | 7.12 | 0.31 | |||
| IVF & ICSI | 1.01 [0.87–1.18] | 55.43 | 26.92 | 0.10 | |||
| LBR | IVF | 0.35 [0.03–4.43] | 0.00 | 0.00 | 0.00 | 1.91 | 0.380 |
| ICSI | 1.05 [0.75–1.47] | 0.00 | 2.54 | 0.47 | |||
| IVF & ICSI | 1.25 [1.14–1.36] | 84.71 | 69.87 | 0.00 | |||
| IR | IVF | 0.59 [0.15–2.32] | 100 | 0.00 | 0.00 | 2.77 | 0.250 |
| ICSI | 0.99 [0.76–1.28] | 0.00 | 0.02 | 0.99 | |||
| IVF & ICSI | 0.77 [0.67–0.89] | 67.03 | 9.10 | 0.03 | |||
| FR | IVF | 0.74 [0.54–1.00] | 0.00 | 0.42 | 0.52 | 10.82 | 0.001 |
| ICSI | 1.09 [0.94–1.26] | 0.00 | 0.79 | 0.37 | |||
| IVF & ICSI | 0.85 [0.82–0.89] | 68.15 | 6.28 | 0.04 | |||
The meta-analysis results revealed variations in miscarriage risk among women with TAI based on the type of assisted reproductive method. Specifically, women undergoing IVF had a 35% higher risk of miscarriage compared to healthy women undergoing IVF (OR: 1.35, 95% CI: 0.56–3.23). In contrast, women undergoing ICSI had a 21% higher risk of miscarriage compared to healthy women undergoing ICSI (OR: 1.21, 95% CI: 0.83–1.76). However, the difference in miscarriage risk between TAI patients undergoing IVF and those undergoing ICSI was not statistically significant (Q = 1.09, p = 0.580). These findings indicate that while TAI may influence miscarriage risk in ART, the type of ART method does not significantly alter this effect (Table 3).
The meta-analysis revealed differences in LBR among women with TAI based on the type of assisted reproductive method. Specifically, women undergoing IVF had a 65% lower chance of live birth compared to healthy women undergoing IVF (OR: 0.35, 95% CI: 0.03–4.43). In contrast, women undergoing ICSI exhibited a 5% higher chance of live birth compared to healthy women undergoing ICSI (OR: 1.05, 95% CI: 0.75–1.47). However, the difference in LBRs between TAI patients undergoing IVF and those undergoing ICSI was not statistically significant (Q = 1.91, p = 0.380). These findings suggest that while the type of ART may influence outcomes, the observed variations were not statistically meaningful in this analysis (Table 3).
The meta-analysis examined the IR among women with TAI based on the type of assisted reproductive method. In women undergoing IVF, the IR was 41% lower compared to healthy women undergoing IVF (OR: 0.59, 95% CI: 0.15–2.32). In women undergoing ICSI, the IR was 1% lower compared to healthy women undergoing ICSI (OR: 0.99, 95% CI: 0.76–1.28). However, the difference in IRs between TAI patients undergoing IVF and those undergoing ICSI was not statistically significant (Q = 2.77, p = 0.250). These findings indicate no meaningful differences in implantation outcomes based on the type of ART among women with TAI (Table 3).
The meta-analysis assessed FR in women with TAI based on the type of assisted reproductive method. Among women undergoing IVF, the FR was 26% lower compared to healthy women undergoing IVF (OR: 0.74, 95% CI: 0.54–1.00). Conversely, in women undergoing ICSI, the FR was 9% higher compared to healthy women undergoing ICSI (OR: 1.09, 95% CI: 0.94–1.26). The difference in FRs between TAI patients undergoing IVF and those undergoing ICSI was statistically significant (Q = 10.82, p = 0.001). These results highlight a notable variation in fertilization outcomes based on the type of ART in women with TAI (Table 3).
This meta-analysis aimed to clarify the association between TAI and ART outcomes. While TAI is often linked to subclinical hypothyroidism and broader immune dysregulation that may impair fertility, our findings indicate a more nuanced picture. Specifically, our analysis revealed statistically significant reductions in implantation and FRs among TAI-positive women, suggesting a potential early impact on reproductive success. However, no significant associations were observed for CPR, LBR, or MR, underscoring the complexity of interpreting TAI’s overall clinical influence. TAI, driven by genetic and epigenetic factors, is primarily seen in women of reproductive age and is characterized by the presence of TPOAb and/or TgAb [52]. Previous studies have extensively examined the impact of TAI on ART outcomes, with some reporting lower CPRs, higher MRs, and reduced LBRs in women with TAI undergoing ART [53, 54]. However, several meta-analyses and comprehensive reviews have found no significant adverse effects of TAI on ART outcomes [55, 56, 57]. One possible explanation for these conflicting findings is the increased use of ICSI in ART. ICSI involves the direct injection of sperm into the egg, bypassing barriers such as the zona pellucida that may otherwise be affected by thyroid antibodies [51]. This technique may reduce the potential negative impact of thyroid autoantibodies on fertilization, which could explain why certain studies have failed to show significant associations between TAI and adverse ART outcomes. Despite the lack of statistically significant findings in our analysis regarding CPR, LBR, and MRs, our results suggest that TAI might still influence earlier stages of reproduction, such as implantation and fertilization. Given the complexity of the relationship between TAI and ART outcomes, further research is necessary to clarify the underlying mechanisms and to determine whether TAI monitoring or targeted treatment strategies may benefit women undergoing ART. Currently, most infertile couples undergo ART, including IVF and ICSI. Spontaneous pregnancies and pregnancies achieved after ART are complicated by miscarriage in 20%–30% of the women. Different risk factors of miscarriage such as genetic, infectious, hormonal, anatomic, and environmental factors have been previously identified [16, 58]. In one study, euthyroid women with TAI characteristics and women with thyroid dysfunction (subclinical) have been identified as having an increased risk of miscarriage [59]. However, other studies have investigated this association in pregnancies following ART and have yielded conflicting data [60, 61, 62, 63].
The present meta-analysis aimed to update the assessment of the impact of the euthyroid phenomenon on pregnancy outcomes in euthyroid women and to compare it with healthy women undergoing ART. Observations have reported contradictory results regarding the impact of TAI on various outcomes. Some studies indicated that the presence of TPOAb is not associated with increased miscarriage or lower birth rates [35, 51, 64]. Conversely, one study has suggested that the presence of elevated TPOAb titers, independent of other organ-specific antibodies, increases the risk of miscarriage following IVF [65]. Additionally, patients with recurrent IVF failure have a higher incidence of TAI, even in the presence of euthyroidism [66, 67].
The meta-analysis by Venables et al. (2020) [68] on TAI and IVF/ICSI outcomes in euthyroid women, as well as the findings by Zhang et al. (2023) [52] regarding high levels of TPOAb as a potential risk factor for adverse pregnancy outcomes, indicate that TAI itself does not significantly affect pregnancy processes in euthyroid women undergoing ART. These results align with our own findings, as our meta-analysis also did not show a significant difference between euthyroid and non-euthyroid groups undergoing ART. However, the meta-analyses conducted in 2016 and the updated 2022 review did reveal significant associations between TAI and an increased risk of miscarriage among euthyroid women undergoing ART [5, 23]. These discrepancies highlight the complexity of the relationship between TAI and ART outcomes, suggesting that factors beyond thyroid function may be at play, such as immune system dysregulation. Further research is needed to explore these nuances and provide more clarity on the specific roles of thyroid antibodies in reproductive health and ART success.
One potential explanation for the inconsistencies in findings regarding the impact of TAI on ART outcomes could be the differences in the classification or grouping of positive and negative TAI cases. The definition of TAI often varies, including the presence of TPOAb alone (in combination with TgAb), or with differing thresholds for what constitutes a positive result. As shown in Fig. 2, no significant difference was observed in the CPR between euthyroid and non-euthyroid women undergoing ART. This result is consistent with previous updates of the same study from 2016 and 2022. Additionally, these findings align with the 2022 meta-analysis by d’Assunção et al. [69], titled “Effect of thyroid function on assisted reproduction outcomes in euthyroid infertile women: A single center retrospective data analysis and a systematic review and meta-analysis”. However, they contrast with the findings of Teixeira et al. [70], who reported a decrease in pregnancy rates among euthyroid women with TAI undergoing ART.
According to the guidelines of the American Association of Clinical Endocrinologists (AACE) and the American Thyroid Association (ATA), the upper limit of TSH should ideally be 2.5 mIU/L during the preconception period and during the first trimester, for the diagnosis and treatment of subclinical hypothyroidism in women planning pregnancy. This recommendation reflects the physiological interaction between human chorionic gonadotropin (hCG) and TSH receptors, which naturally lowers TSH levels during early pregnancy [71].
Moreover, no significant difference was observed in the comparison of LBRs
between the two groups under investigation. Review studies suggest that for women
intending to conceive, serum TSH concentrations should be below 2.5 mIU/L, and
this level should be maintained during the first and second trimesters of
pregnancy. The detrimental effects of elevated TSH levels above the normal range
(
Nevertheless, evidence suggests that variations in TSH levels within the normal range do not, by themselves, significantly impact pregnancy outcomes [73]. TAI, even in a euthyroid state, may negatively affect fertility and pregnancy outcomes by creating a cytotoxic environment that damages mature oocytes, thereby reducing their quality and fertilization potential, and by causing subtle disruptions in the early stages of pregnancy [74]. The present systematic review and meta-analysis demonstrated that women with positive TAI undergoing ART cycles have lower implantation and FRs. This finding has also been consistently reported in other studies. For instance, in a study conducted by Teixeira et al. [70], which systematically reviewed the impact of thyroid disorders on ART clinical outcomes over the past 10 years, demonstrated that thyroid disorders can reduced FRs and the number of viable embryos in both IVF and ICSI procedures.
Other studies have also shown an association between TAI and reduced fertility.
In a review of women with various causes of infertility, Poppe and Glinoer
[59] found a significantly higher incidence of TAI [RR: 2.1, p
Since all the components necessary for thyroid hormones synthesis, including sodium/iodide symporter, pendrin, TPO, and Tg, are present in the endometrium, syncytiotrophoblast, and invasive trophoblast, local synthesis of thyroid hormones is plausible. Under such circumstances, TAI could lead to thyroid hormone deficiency at the tissue level, disrupting the process of embryo implantation and placentation processes, with consequent infertility or obstetrical complications [76].
While a random-effects model was employed to account for heterogeneity across studies, several key outcomes, including CPR, MR, and LBR, did not reach statistical significance. Therefore, although trends were observed favoring the TAI-negative group, these findings should be interpreted with caution. The lack of significance underscores the need for further high-quality, prospective studies to confirm potential associations between TAI and ART outcomes.
The subgroup analyses in the present meta-analysis demonstrated that in women who underwent ICSI or IVF exclusively, there was a significant association in CPRs between women with autoimmune thyroid disease and healthy women undergoing IVF compared to women with autoimmune thyroid disease and healthy women undergoing ICSI (Q = 8.91, p = 0.010). In other words, ARTs were a source of heterogeneity in the desired outcome. Additionally, regarding FRs, a statistically significant difference was observed between women with autoimmune thyroid disease and healthy women undergoing IVF compared to those undergoing ICSI (Q = 10.82, p = 0.001), indicating a source of heterogeneity. However, for the other outcomes examined—MR, IR, and LBR—no significant differences were observed between women with autoimmune thyroid disease and healthy women across IVF and ICSI groups. In these outcomes, ART was not a source of heterogeneity.
This study has several strengths. First, by establishing strict inclusion and exclusion criteria, we controlled for potential confounding factors, such as other autoantibodies and severe detrimental elements. This minimization of confounders ensured that the focus remained solely on comparing the outcomes of ART in women with TAI and healthy women. Second, only first-time ART users were included in the analysis. This approach allowed us to examine a homogeneous population with a favorable prognosis, thereby providing relevant recommendations for the target population.
While this meta-analysis provides valuable insights into the relationship between TAI and ART outcomes, there are several limitations to consider. First, publication bias may affect the results, as studies with null findings are less likely to be published. This could lead to an overestimation of the true effect size. Funnel plot analyses and Egger’s test were conducted to assess for publication bias, but it remains a potential limitation, especially given the observational nature of the included studies. Future research should prioritize publishing studies regardless of outcome to mitigate this bias. Second, confounding factors such as age, underlying health conditions (e.g., polycystic ovary syndrome, endometriosis), and variations in ART protocols could influence ART outcomes. While some studies adjusted for these factors, not all studies controlled for potential confounders in their analyses. Future studies should rigorously control for these variables to better isolate the impact of TAI on ART outcomes. Finally, the validity of the included studies may be affected by methodological differences in how TAI was defined. Some studies included only TPOAb positivity, while others required positivity for both TPOAb and TgAb, or applied varying thresholds for antibody levels. These discrepancies may have led to inconsistencies in the results. Additionally, different ART protocols and outcome measures across studies further complicate the interpretation of the findings. Standardizing these definitions in future research would enhance the comparability and validity of the findings. It is important to differentiate between TAI in euthyroid women (normal free thyroid hormone and TSH levels) and TAI accompanied by abnormal thyroid function. This analysis did not consistently stratify results based on thyroid function status beyond TAI antibody positivity; therefore, future studies should explore this distinction to better clarify the reproductive impact of thyroid function versus antibody status alone. Moreover, given the lack of effective treatment options for TAI in euthyroid women undergoing ART, future research should focus on identifying the specific immunological mechanisms by which TAI may affect fertility, even in the absence of overt thyroid dysfunction. Prospective, large-scale studies are also needed to determine whether targeted immunomodulatory therapies can improve ART outcomes in this population.
TAI is frequently associated with subtle immune dysfunctions that may impact reproductive processes, though the exact clinical significance remains unclear. While this meta-analysis observed lower IRs and FRs in women with TAI undergoing ART, no statistically significant differences were found for LBR, CPR, or MR. These findings suggest that TAI may affect early reproductive outcomes, but its overall impact on successful pregnancy remains inconclusive. Variability in study design, patient populations, and diagnostic assays across the included studies likely contributed to the observed heterogeneity in the results. A deeper understanding of the immunological mechanisms underlying TAI and well-designed prospective studies are essential to clarify its role in ART outcomes and guide future clinical management.
TSH, thyroid-stimulating hormone; TAI, thyroid autoimmunity; TPOAb, thyroid peroxidase antibodies; IL, interleukin; IFN-
All data generated or analyzed during this study are available from the corresponding author upon reasonable request.
YM conceptualized the study, formulated the research objectives, developed the methodology, contributed to data analysis and interpretation, and led the manuscript writing. HG co-developed the study design, supported methodological refinement, assisted with data interpretation, and contributed to manuscript drafting. ZH formulated the research questions and contributed to the conceptual framework. JA conducted data extraction and contributed to data analysis. EN performed data extraction and supported quality assessment. LS contributed to data extraction, participated in the risk of bias assessment and supported language editing and clarity of presentation. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study was approved by the Ethics Committee of Kurdistan University of Medical Sciences (Approval Code: IR.MUK.REC.1402.039). The manuscript is derived from a medical doctoral thesis conducted as part of the General Medicine program.
The authors would like to express their sincere gratitude to all colleagues and staff who supported this study. We especially acknowledge Mostafa Zarei for his assistance with the registration process and administrative coordination.
This research received no external funding.
The authors declare no conflict of interest.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG37060.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.