
Academic Editor: Luca Roncati
Background: Medicine is to some extent an empirical science that
requires repeated clinical practice. To explore the needs of obstetricians &
gynecologists (Ob & Gy) in different kinds of hospitals for continuing medical education
(CME) training content and forms. Method: From April 2020 to May 2020,
an online questionnaire was distributed on the largest academic training platform
for Ob & Gy in China, which included doctors’
mastery of diseases, training content and forms of CME. Results: A total
of 4458 questionnaires were returned, of which 3954 were included in the study.
There is a significant statistical difference between doctors in general
hospitals, maternity specialized hospitals, or maternity and child specialized
hospitals in the mastery of most common gynecological and obstetric diseases,
among which, doctors in general hospitals have a better mastery (p
Continuing medical education (CME) refers to the lifelong education of continuing to learn relevant new theories, methods and technologies within the specialty after completing basic medical education, postgraduate education, and professional training for residents [1]. A multi-level medical education system for the training of medical practitioners has always been adopted in China [2], and there are great differences in the growth environment of medical students after practice, which leads to the otherness of Chinese doctors. Multiple training needs make CME only rely on a flexible and open lifelong education system to meet personalized requirements because the professional background, educational level, work experience, and working environment of doctors are very different [3, 4].
Hospitals in China are divided into general hospitals, specialized hospitals, clinics, etc. A general hospital refers to the medical institution providing medical services for general practice or main general subjects, in which, all-around medical and health services can be provided with relatively complete departments [5]. A specialized hospital refers to a hospital that treats diseases in a system or age group and has certain limitations on the scope of diseases admitted, such as obstetrics and gynecology hospital, children’s hospital, and so on. A clinic is a medical institution that can only provide outpatient services for common diseases, and the size of the clinic is generally relatively small. Doctors working in general hospitals and specialized hospitals are the main group of practitioners. This paper mainly investigates and analyzes the needs of obstetricians & gynecologists (Ob & Gy) in a general hospital and Maternity and children hospital or reproductive hospital (hereinafter referred to as specialized hospitals) for continuing education, and provides evidence for carrying out targeted CME in hospitals of different types, and strives to improve the effect of CME.
The online questionnaire was distributed on the largest academic training platform for obstetrics & gynecology in China from April 2020 to May 2020 by using the survey method of an online questionnaire. Gynecology-related training videos were given free of charge to doctors who completed the questionnaire, to encourage more doctors to participate in the survey.
The survey content of the questionnaire is mainly aimed at the needs of Ob & Gy for training content and training methods, and at the same time, the survey content of the questionnaire is adjusted according to the characteristics of the discipline setting to make it meet the actual situation of medical institutions in China. The content and design of the questionnaire were discussed and amended by the expert group and validated among small-scale Ob & Gy before being released on the web platform.
The study was reviewed and approved by the Ethics Review Committee of the Peking Union Medical College Hospital, Chinese Academy of Medical Sciences on 8 June, 2020 (number S-K 1206).
Chinese Ob & Gy participated in the survey with inclusion criteria of clinicians in obstetrics & gynecology or reproductive specialty, and exclusion criteria of doctors who are not from obstetrics & gynecology and reproductive specialty, insufficient basic information in the submitted questionnaire, incompletion of the survey content in the submitted questionnaire, obvious logical errors in the submitted questionnaire, and contradictory content filling.
The content of the questionnaire is mainly aimed at common diseases in obstetrics & gynecology, and assesses the mastery of diseases by Ob & Gy and the expected training content and training methods. The questionnaire was developed and reviewed by four specialists in reproductive endocrinology and obstetrics & gynecology. 30 Ob & Gy were first invited to fill in the designed questionnaire, and the questionnaire was distributed in the network after confirming that there were no omissions.
Basic demographic data, mainly including age, gender, specialized department, working years, types of hospitals and hospital level (first-level, second-level, tertiary-level and others).
The survey on training content mainly has the professional direction (multiple choices) that the respondent most hopes to strengthen training, including common gynecological endocrine diseases, common gynecological diseases, common obstetrical diseases, surgical skills training and others, and the training content that the respondent most wants to listen to (multiple choices), including abnormal uterine bleeding (AUB), and so on.
The survey on training forms mainly includes the favorite training forms, the most beneficial training modes, the ways to obtain professional-related resources and support (optional). Problem-based learning (PBL) is a problem-based learning process in which questions are proposed, discussed, and learned around a complex, multi-scene, practical problem-based topic or case with the participation and guidance of counselors, the core of which is problem-centered, with student discussion as the main body and teachers as guides [4].
A survey on the knowledge about disease diagnosis and treatment, including a total of 19 common diseases such as AUB, amenorrhea, and other gynecological and obstetric-related diseases. The mastery of knowledge is classified into four levels, including hardly understand, understand small parts, be familiar with the most, and master comprehensively.
SPSS 22.0 software (IBM Corp., Chicago, IL, USA) was used for statistical
analysis of the data. In this survey, general demographic data (such as age,
gender, etc.) and doctors’ selection of training content, training form and way
to obtain professional support were expressed as percentages or n (%).
Univariate analysis was performed using the
A total of 4458 questionnaires were returned, of which 3954 met the inclusion and were included in the study report. The main reason for exclusion was non-Ob & Gy, such as health care physicians, nurses, sonographers, administrative personnel, teachers, etc., in addition, questionnaires with the same answer for all questions were excluded.
Among the valid questionnaires, Ob & Gy and gynecologist
accounted for the highest proportion, followed by obstetricians, and
reproductive/gynecological endocrinologists accounted for the least proportion.
Among general hospitals and specialized hospitals, 18–25 years old was the age
group with the least number of participants, the age group with the highest
number of participants was 36–45 years old, doctors from working years
| Category | n (%) | Maternity and children hospital or reproductive hospital | General hospitals | Others | |
|---|---|---|---|---|---|
| Total number | 3954 | 1593 (40.29) | 2210 (55.89) | 151 (3.82) | |
| Gender | Female | 3860 (97.62) | 1554 (97.55) | 2156 (97.56) | 150 (99.34) |
| male | 94 (2.38) | 39 (2.45) | 54 (2.44) | 1 (0.66) | |
| Age groups (years) | 18–25 | 39 (0.99) | 23 (1.44) | 15 (0.68) | 1 (0.66) |
| 26–35 | 701 (17.73) | 255 (16.01) | 425 (19.23) | 21 (13.91) | |
| 36–45 | 1677 (42.41) | 651 (40.87) | 967 (43.76) | 59 (39.07) | |
| 46–55 | 1357 (34.32) | 596 (37.41) | 697 (31.54) | 64 (42.38) | |
| 180 (4.55) | 68 (4.27) | 106 (4.80) | 6 (3.97) | ||
| Specialty type | Obstetrician | 337 (8.52) | 156 (9.79) | 178 (8.05) | 3 (1.99) |
| Gynecologist | 1164 (29.44) | 539 (33.84) | 571 (25.84) | 54 (35.76) | |
| Obstetrician–gynecologist | 2289 (57.89) | 796 (49.97) | 1401 (63.39) | 92 (60.93) | |
| Reproductive endocrinologist | 164 (4.15) | 102 (6.40) | 60 (2.71) | 2 (1.32) | |
| Year of work (year) | 274 (6.93) | 114 (7.16) | 154 (6.97) | 6 (3.97) | |
| 6–10 | 524 (13.25) | 190 (11.93) | 308 (13.94) | 26 (17.22) | |
| 11–20 | 1205 (30.48) | 461 (28.94) | 708 (32.04) | 36 (23.84) | |
| 1951 (49.34) | 828 (51.98) | 1040 (47.06) | 83 (54.97) | ||
| Hospital level | First hospital | 425 (10.75) | 77 (4.83) | 274 (12.40) | 74 (49.01) |
| Secondary hospital | 2049 (51.82) | 893 (56.06) | 1139 (51.54) | 17 (11.26) | |
| Tertiary hospital | 1078 (27.26) | 392 (24.61) | 673 (30.45) | 13 (8.61) | |
| Others | 402 (10.17) | 231 (14.50) | 124 (5.61) | 47 (31.13) |
The mastery of 19 diseases was divided into two major types: low cognition (be
familiar with hardly understand and understand small parts), and high cognition
(be familiar with the most and master comprehensively). As a result, the judgment
criteria were considered as a better stratification of disease mastery with high
cognition
The proportion of doctors in specialized hospitals and general hospitals who
achieved high cognition of common gynecological and obstetric diseases was
Univariate chi-square analysis showed that the mastery of 19 diseases was statistically different in the majority of Ob & Gy in different types of hospitals. The mastery (high cognition) of 19 diseases of Ob & Gy in different types of hospitals is shown in Table 2 and Fig. 1.
| Diseases | Maternity and children hospital or reproductive hospital | General hospital | Others | X |
p |
|---|---|---|---|---|---|
| AUB | 925 (58.07) | 1391 (62.94) | 80 (52.98) | 13.03 | 0.001 |
| Amenorrhea | 784 (49.22) | 1142 (51.67) | 65 (43.05) | 5.59 | 0.061 |
| PCOS | 757 (47.52) | 1101 (49.82) | 58 (38.41) | 8.30 | 0.016 |
| Infertility | 495 (30.17) | 604 (27.33) | 32 (21.19) | 10.57 | 0.005 |
| Menopausal syndrome | 686 (43.06) | 931 (42.13) | 57 (37.75) | 1.69 | 0.430 |
| Precocious puberty/CDP | 212 (13.31) | 218 (9.86) | 13 (8.61) | 12.10 | 0.002 |
| Hyperprolactinemia | 375 (23.54) | 515 (23.30) | 24 (15.89) | 4.64 | 0.098 |
| Premature ovarian failure | 542 (34.02) | 705 (31.90) | 36 (23.84) | 7.21 | 0.027 |
| HPV infection and cervical lesions | 1057 (66.35) | 1487 (67.29) | 90 (59.60) | 3.83 | 0.147 |
| Leiomyoma | 1136 (71.31) | 1768 (80.0) | 98 (64.90) | 48.66 | |
| Ovarian cyst | 882 (55.37) | 1504 (68.05) | 64 (42.38) | 88.75 | |
| Endometriosis | 776 (48.71) | 1290 (58.37) | 57 (37.75) | 50.78 | |
| Family planning (contraception/IUD/abortion) | 1307 (82.05) | 1888 (85.43) | 114 (75.50) | 15.48 | |
| Routine labor management | 1131 (71.0) | 1758 (79.55) | 86 (56.95) | 64.50 | |
| Pregnancy-induced hypertension syndrome | 1000 (62.77) | 1583 (71.63) | 76 (50.33) | 53.35 | |
| Gestational diabetes mellitus | 799 (50.16) | 1312 (59.37) | 55 (36.42) | 53.05 | |
| Premature rupture of membranes | 1090 (68.42) | 1716 (77.65) | 85 (56.29) | 62.67 | |
| Premature delivery | 1014 (63.65) | 1606 (72.67) | 76 (50.33) | 57.76 | |
| Gemellary pregnancy | 806 (50.60) | 1298 (58.73) | 54 (35.76) | 47.14 | |
| AUB, Abnormal uterine bleeding; HPV, Human papillomavirus; PCOS, Polycystic ovary syndrome; CDP, Constitutional delay of puberty; IUD, Intrauterine device. | |||||
 Fig. 1.
Fig. 1.The mastery (high cognition) of 19 diseases of Ob & Gy in different types of hospitals.
After adjusting age, specialty type, working years and hospital level, a regression analysis of the effect of Ob & Gy in different types of hospitals on the mastery of 19 diseases have been made. With specialized hospitals as the reference, the results showed that except for the mastery of human papillomavirus (HPV) infection and cervical lesions was not significantly different between specialized hospitals and general hospitals (p = 0.61), the mastery of other common gynecological and obstetric diseases was higher in doctors in general hospitals than those in specialized hospitals, and the difference was statistically significant. However, there was no significant difference in the mastery of gynecological endocrine-related diseases between specialized hospitals and general hospitals for amenorrhea, Polycystic ovary syndrome (PCOS), menopausal syndrome, hyperprolactinemia, premature ovarian failure; doctors in general hospitals were higher than those in specialized hospitals in the mastery of AUB and lower than those in specialized hospitals in the mastery of precocious puberty/Constitutional delay of puberty (CDP) and infertility, both of which were statistically significant. Analysis of the difference in mastery of 19 diseases by doctors in different types of hospitals after adjusting for multiple factors is presented in Tables 3,4,5,6,7.
| Hospital type | AUB | Amenorrhea | PCOS | Infertility | ||||
|---|---|---|---|---|---|---|---|---|
| Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | |
| Maternity and children hospital or reproductive hospital | 1.00 | 1.00 | 1.00 | 1.00 | ||||
| General hospital | 1.25 (1.09 |
0.00 | 1.12 (0.97 |
0.12 | 1.07 (0.94 |
0.32 | 0.80 (0.69 |
0.00 |
| Others | 0.83 (0.58 |
0.29 | 0.78 (0.55 |
0.18 | 0.72 (0.51 |
0.07 | 0.61 (0.40 |
0.02 |
| AUB, Abnormal uterine bleeding; PCOS, Polycystic ovary syndrome; CI, Confidence Interval. | ||||||||
| Menopausal syndrome | Precocious puberty / CDP | Hyperprolactinemia | Premature ovarian failure | ||||
|---|---|---|---|---|---|---|---|
| Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p |
| 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 0.98 (0.86 |
0.82 | 0.71 (0.58 |
0.00 | 0.96 (0.82 |
0.58 | 0.89 (0.77 |
0.13 |
| 0.79 (0.55 |
0.20 | 0.63 (0.35 |
0.13 | 0.64 (0.40 |
0.06 | 0.61 (0.41 |
0.02 |
| CDP, Constitutional delay of puberty; CI, Confidence Interval. | |||||||
| HPV infection and cervical lesions | Leiomyoma | Ovarian cyst | Endometriosis | ||||
|---|---|---|---|---|---|---|---|
| Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p |
| 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 1.04 (0.90 |
0.61 | 1.56 (1.33 |
0.00 | 1.66 (1.45 |
0.00 | 1.44 (1.26 |
0.00 |
| 0.78 (0.55 |
0.15 | 0.82 (0.57 |
0.29 | 0.65 (0.46 |
0.02 | 0.70 (0.49 |
0.05 |
| HPV, Human papillomavirus; CI, Confidence Interval. | |||||||
| Family planning (contraception/ IUD/abortion) | Routine labor management | Pregnancy-induced hypertension syndrome | Gestational diabetes mellitus | ||||
|---|---|---|---|---|---|---|---|
| Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p |
| 1.00 | 1.00 | 1.00 | 1.00 | ||||
| 1.35 (1.12 |
0.00 | 1.54 (1.32 |
0.00 | 1.46 (1.26 |
0.00 | 1.39 (1.22 |
0.00 |
| 0.64 (0.42 |
0.03 | 0.56 (0.40 |
0.00 | 0.64 (0.46 |
0.01 | 0.63 (0.44 |
0.01 |
| IUD, Intrauterine device; CI, Confidence Interval. | |||||||
| Premature rupture of membranes | Premature delivery | Gemellary pregnancy | |||
|---|---|---|---|---|---|
| Exp (B) (95% CI) | p | Exp (B) (95% CI) | p | Exp (B) (95% CI) | p |
| 1.00 | 1.00 | 1.00 | |||
| 1.53 (1.31 |
0.00 | 1.47 (1.27 |
0.00 | 1.38 (1.20 |
0.00 |
| 0.64 (0.45 |
0.01 | 0.62 (0.44 |
0.00 | 0.58 (0.40 |
0.00 |
| CI, Confidence Interval. | |||||
For the professional direction of hoping to strengthen training, specialized hospitals and general hospitals had the highest choice for common gynecological endocrine diseases, the second choice for general hospitals was surgical technique training, while specialized hospitals had the second choice for common gynecological diseases. Common obstetric disorders were the least selected training directions. The top three training content for general hospitals and specialized hospitals were the same, which were AUB, menopausal syndrome and PCOS. In both specialized and general hospitals, the favorite training forms were network + on-site training, the training model with the greatest gain was a situational simulation, and the online course was the most selected as the way to obtain professional resources and support. Investigation of the training content, training forms and ways to obtain professional support of Ob & Gy in different types of hospitals are shown in Table 8 and Figs. 2,3.
| Training and professional support | Total number | Maternity and children hospital or reproductive hospital | General hospital | Others | |
| n = 1593 | n = 2210 | n = 151 | |||
| The respondent most hopes to strengthen training | Common gynecological endocrine diseases | 3221 (81.46) | 1303 (81.80) | 1797 (81.31) | 121 (80.13) |
| Common gynecological diseases | 1474 (37.28) | 643 (40.36) | 740 (33.48) | 91 (60.26) | |
| Common obstetrical diseases | 650 (16.44) | 271 (17.01) | 351 (15.88) | 28 (18.54) | |
| Surgical skills training | 1570 (39.71) | 540 (33.90) | 1005 (45.48) | 25 (16.56) | |
| Others | 71 (1.80) | 27 (1.69) | 38 (1.72) | 6 (3.97) | |
| The respondent most wants to listen to | AUB | 3359 (84.95) | 1350 (84.75) | 1876 (84.89) | 133 (88.08) |
| Menopausal syndrome | 2849 (72.05) | 1142 (71.69) | 1587 (71.81) | 120 (79.47) | |
| PCOS | 2508 (63.43) | 1006 (63.15) | 1419 (64.21) | 83 (54.97) | |
| Infertility | 2318 (58.62) | 979 (61.46) | 1259 (56.97) | 80 (52.98) | |
| EM & AM | 2053 (51.92) | 831 (52.17) | 1144 (51.76) | 78 (51.66) | |
| Leiomyoma & Ovarian cyst | 1493 (37.76) | 608 (38.17) | 819 (37.06) | 66 (43.71) | |
| Cervical lesions | 2306 (58.32) | 924 (58.00) | 1285 (58.14) | 97 (64.24) | |
| Obstetric-related diseases | 1476 (37.33) | 593 (37.23) | 836 (37.83) | 47 (31.13) | |
| Favorite training forms | Online | 1827 (46.21) | 708 (44.44) | 1049 (47.47) | 70 (46.36) |
| On-site meeting report | 186 (4.70) | 83 (5.21) | 95 (4.30) | 8 (5.30) | |
| Network + on-site training | 1941 (49.09) | 802 (50.35) | 1066 (48.24) | 73 (48.34) | |
| The most beneficial training modes | Traditional lecture | 1266 (32.02) | 503 (31.58) | 702 (31.76) | 61 (40.40) |
| PBL mode | 889 (22.48) | 354 (22.22) | 500 (22.62) | 35 (23.18) | |
| Scenario simulation | 1799 (45.50) | 736 (46.20) | 1008 (45.61) | 55 (36.42) | |
| Ways to obtain professional-related resources and support | Regular WeChat push | 3225 (81.56) | 1287 (80.79) | 1809 (81.86) | 129 85.43) |
| Professional website | 2034 (51.44) | 822 (51.60) | 1135 (51.36) | 77 (50.99) | |
| Meeting or forum | 1740 (44.01) | 703 (44.13) | 973 (44.03) | 64 (42.38) | |
| Online course | 3010 (76.13) | 1206 (75.71) | 1684 (76.20) | 120 (79.47) | |
| AUB, Abnormal uterine bleeding; PCOS, Polycystic ovary syndrome; PBL, Problem-based learning; EM, Endometriosis; AM, Adenomyosis. | |||||
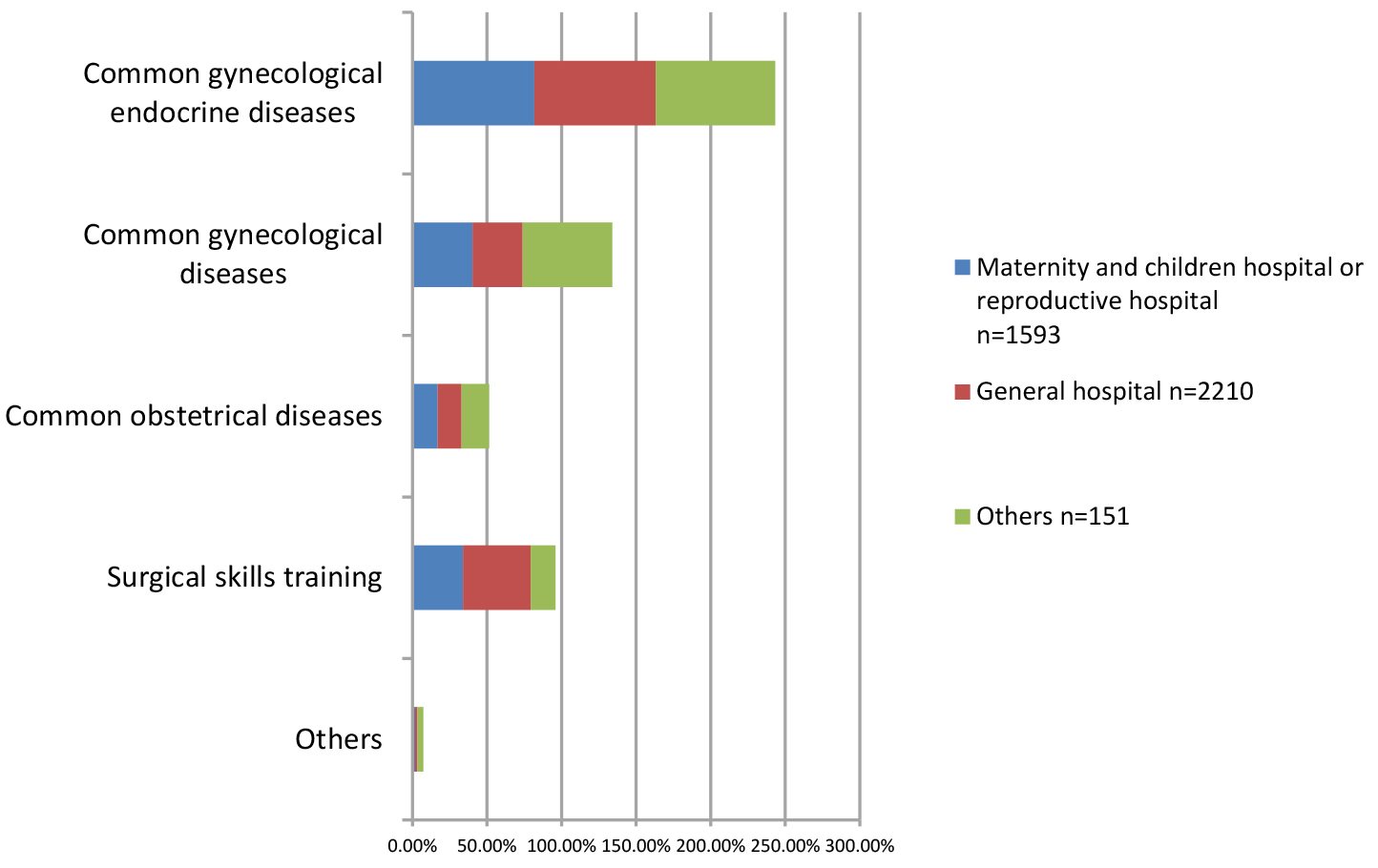 Fig. 2.
Fig. 2.Investigation of the areas of specialist training that Ob & Gy in different types of hospitals would like to strengthen.
 Fig. 3.
Fig. 3.Investigation of the training content which are most desired by Ob & Gy in different types of hospitals. AUB, Abnormal uterine bleeding; PCOS, Polycystic ovary syndrome.
Based on the results of our survey, the mastery of diseases by Ob & Gy was related to the type of hospital which they work for. The mastery of diseases in general hospitals, specialized hospitals and other kinds of hospitals showed a decreasing trend; the mastery of gynecological endocrine-related diseases by doctors in different types of hospitals was generally lower than that of common gynecological and obstetric diseases. After adjusting working years, hospital level and other related factors, it was found that for the mastery of common gynecological and obstetric diseases, except that HPV infection/cervical lesions had no significant difference among different types of hospitals, general hospitals were significantly higher than specialized hospitals, and other types of hospitals had the lowest mastery of diseases. Analyzing the possible causes: the statistical data of China in 2015 showed that the incidence and mortality of cervical cancer were 98.9/100,000 and 30.5/100,000, respectively. Compared with the decreased incidence in developed countries, the incidence and mortality of cervical cancer in China showed an increasing trend [6, 7, 8]. It is possible that there is no significant statistical difference between different kinds of hospitals due to the relatively simple condition of HPV infection/cervical lesions, large clinical need and sufficient CME for them [8].
Specialized hospitals are characterized by specialty technical advantages, but the technical strength of other disciplines is relatively weak. The diagnosis and treatment ability of specialized hospitals for patients with complications or complex and critical diseases is significantly weaker than that of general hospitals [9]. Many diseases in obstetrics & gynecology department and the patient population are often complicated with other systemic diseases at the same time, such as pregnant women complicated with various diseases, and elderly patients may be complicated with cardiovascular diseases, nephropathy and endocrine diseases. Therefore, many patients with complications or complex conditions choose to go to general hospitals for diagnosis and treatment, which makes specialized hospitals more opportunities to see patients with a single and no complications. The difference in the treatment of patients will certainly affect doctors’ level of diagnosis and treatment of diseases.
Doctors in different types of hospitals generally have lower mastery of gynecological endocrine-related diseases than common gynecological and obstetric diseases and have different mastery of different diseases. After adjusting related factors, it was found that the mastery of AUB in general hospitals was better than that in specialized hospitals, while in terms of infertility and precocious puberty, specialized hospitals were better than general hospitals. Analyzing the possible reasons: AUB can be caused by a variety of reasons and is a common reason for outpatient and emergency visits to women of childbearing age [10]. General hospitals have the advantage of multi-disciplinary cooperation in the treatment of complex and complicated diseases, so the diagnosis and treatment ability is higher. Infertility and precocious puberty are diseases that required highly specialized knowledge, and the advantage lay with the targeted special medical services of specialized hospitals. Training directions hoped to be strengthened and the training content that most wanted is consistent with the doctors’ mastery of diseases. Doctors in different kinds of hospitals prefer common gynecological endocrine diseases. AUB, menopausal syndrome and PCOS are the top three diseases selected.
From our findings, the training form and the way to obtain professional resources with the help of the network are the most popular models. Since the World Health Organization announced Coronavirus disease 2019 (COVID-19) as a pandemic on 11 March, 2020, due to the dramatic increase in global incidence, more and more learners have been forced to switch to e-learning models using networks, both medical education for undergraduate students [11, 12] and CME for practitioners [13]. Internet education has the advantages of relatively low cost, higher flexibility, freedom from geographical location, rapid content update, and individualized selection of learning content, but it also lacks communication and interaction between learners and teachers, as well as between learners, which reduces learning motivation and needs more self-discipline [14].
In summary, from our investigation results, in China, doctors in general hospitals have a higher mastery of common gynecological and obstetric diseases than doctors in specialized hospitals, doctors in different types of hospitals generally have a lower mastery of gynecological endocrine-related diseases. So the most preferred training direction and training content Ob & Gy in different types of hospitals were gynecological endocrine-related diseases. Using the Internet is the most popular educational model, however, further study needed to be conducted as to whether the effect of Internet education is better than that of the traditional educational model.
Not applicable.
The datasets used and/or analysed during the current study are available from the corresponding author upon reasonable request.
HW and AS contributed to wrote and edited the manuscript, the data collection, interpretation and analysis. AS contributed to the conceptualization and design of the study. JC, HD, YZ, WW, QZ, YF and ZT contributed to the data collection. ZT, XZ, YZ and YW contributed to the protocol planning, data collection and analysis. ZZ, ZT, XZ, YZ and YW contributed to patient recruitment and data collection. All authors read and approved the final version of the paper.
This trial was approved by the Ethics Committee of Peking Union Medical College Hospital, Peking Union Medical College, Chinese Academy of Medical Science (No. S-K 1206). All participants provided written informed consent.
Not applicable.
This work was supported by the Capital’s Funds for Health Improvement and Research (CFH:2020-2-40113) and the National Natural Science Foundation (Grant number: 82074143). Dr. Aijun Sun received the research grant.
The authors declare no conflict of interest.
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.