


 , Luca Sarchi 1,2, Marco Paciotti 1,2,5,6, Carlo Andrea Bravi 1,2,7, Angelo Mottaran 1,2,8,9, Adele Piro 10, Luigi Nocera 7, Tommaso Calcagnile 10, Simone Assumma 10, Maria Chiara Sighinolfi 10, Siddhart Yadav 11, Stefano Terzoni 12, Stefano Puliatti 10, Periklis Koukourikis 13, Ruben De Groote 1,2, Fátima Faustino 14, Geert De Naeyer 1,2, Giorgia Gaia 15, Bernardo Rocco 16, Alexandre Mottrie 1,2
, Luca Sarchi 1,2, Marco Paciotti 1,2,5,6, Carlo Andrea Bravi 1,2,7, Angelo Mottaran 1,2,8,9, Adele Piro 10, Luigi Nocera 7, Tommaso Calcagnile 10, Simone Assumma 10, Maria Chiara Sighinolfi 10, Siddhart Yadav 11, Stefano Terzoni 12, Stefano Puliatti 10, Periklis Koukourikis 13, Ruben De Groote 1,2, Fátima Faustino 14, Geert De Naeyer 1,2, Giorgia Gaia 15, Bernardo Rocco 16, Alexandre Mottrie 1,21 ORSI Academy, 9090 Melle, Belgium
2 Department of Urology, OLV, 9300 Aalst, Belgium
3 Urology Department, Centro Hospitalar Universitário de Lisboa Central, 1150-199 Lisbon, Portugal
4 Department of Gynecology, Lusiadas Hospital, 1500-458 Lisbon, Portugal
5 Department of Biomedical Sciences, Humanitas University, 20090 Pieve Emanuele, Italy
6 Department of Urology, IRCCS Humanitas Research Hospital, 20089 Rozzano, Italy
7 Division of Oncology/Unit of Urology, URI, IRCCS Ospedale San Raffaele, 20132 Milan, Italy
8 Division of Urology, IRCCS Azienda Ospedaliero-Universitaria di Bologna, 40138 Bologna, Italy
9 University of Bologna, 40126 Bologna, Italy
10 Department of Urology, University of Modena and Reggio Emilia, 41121 Modena, Italy
11 Department of Urology & Renal Transplant, Vardhman Mahavir Medical College and Safdarjung Hospital, 110029 New Deli, India
12 San Paolo bachelor School of Nursing, ASST Santo Santi Paolo e Carlo, University of Milan, 20122 Milan, Italy
13 Second Department of Urology, Medical School, Aristotle University of Thessaloniki, 541 24 Thessaloniki, Greece
14 Department of Gynecology, Lusíadas Hospital, 1500-458 Lisbon, Portugal
15 Department of Obstetrics and Gynaecology, ASST Santi Paolo e Carlo, University of Milan, 20122 Milan, Italy
16 Urological Unit, Department of Health Sciences, ASST Santi Paolo e Carlo, University of Milan, 20122 Milan, Italy
Academic Editor: Johannes Ott
Abstract
Objective: To summarize the scientific published literature on new robotic platforms with potential use in gynecology and review their evolution from inception until the present day. The goal was to describe the current characteristics and possible prospects of these platforms. Mechanism: A non-systematic search of PubMed, Cochrane Library Central, EMBASE, MEDLINE, and Scopus databases was conducted to identify scientific literature on new robotic platforms and review their evolution from inception until January 2022. Only English-language publications were included in this analysis. The following keywords were used: “new robotic platforms”, “robot”, “Revo-I”, “Versius®”, “Senhance®”, “Single-Site”, “Single-Port”, “Multi-Port”, “EDGE SP1000”, “Flex®”, and “Hominis®”. Abstract reviews were conducted to determine the relevance of the review aims. Full-text analysis of all relevant English-language original articles was subsequently performed by one author (R.F.) and summarized after discussion with an independent third party (L.S., M.P.). No formal quality assessment of the included studies was conducted. Findings in brief: The Da Vinci robotic system is the leading platform in the robotic surgery market. Other new platforms have published peer-reviewed articles in the field of gynecology. Senhance® and Da Vinci SP® have the most substantial proof of their capacity to perform multi-incision and single-incision robotic surgery, respectively. Hominis® has the potential to play a major role in ultra-minimally invasive and scarless approaches. Conclusions: The significant advantages of Intuitive’s robots justify their worldwide dissemination. However, their drawbacks have motivated other companies to develop innovative solutions. Our research shows that the majority of these new platforms are still at the beginning of their technical and scientific validation but seem very promising.
Keywords
- robotic surgery
- REVO-I
- Versius®
- Senhance®
- Single-Site
- Single-Port
- Multi-Port
- EDGE SP1000
- Flex®
- Hominis®
The technical limitations and long learning curve of laparoscopic surgery motivated the contribution of surgical robotic companies to the development of new surgical armamentariums. To date, only a few companies have reached a stage of development that has granted them approval to operate in humans. The current manuscript aims to unveil the new frontier explored by these new devices based on peer-reviewed scientific publications studying their application in gynecology.
A non-systematic search of the PubMed, Cochrane Library’s Central, EMBASE, MEDLINE, and Scopus databases was conducted to identify peer-reviewed articles, showing the use of new robotic platforms in gynecology, reviewing their evolution from inception until January 2022. We aimed to describe their features, as well as preclinical and clinical gynecological studies.
Only English-language publications were included in this analysis. The following keywords were used “new robotic platforms”, “robot”, “Revo-I”, “Versius®”, “Senhance®”, “Single-Incision”, “Multi-Port”, “Single-Site”, “Single-Port”, “EDGE SP1000”, “Flex®”, “Hominis®”. Abstract reviews were conducted to determine the relevance for the review aims. Full-text analysis of all relevant English-language original articles was subsequently performed by one author (R.F.) and summarized after discussion with an independent third party (L.S., M.P.). No formal quality assessment of the included studies was conducted.
The first scientific publications using the Da Vinci robotic surgical system (Intuitive Surgical Mountain View, CA, USA) were published in the 90s [1, 2, 3], after which Intuitive became the leading company in the robotic surgical platform market [4, 5, 6]. Its use in gynecology was approved by the Food and Drug Administration (FDA) in 2005 [7], and its growing popularity among gynecologists and patients has increased the number and range of surgeries performed [7].
However, robotic surgery is relatively uncommon in this surgical specialty. Studies showing that both laparoscopic and robotic approaches are equally safe [8], the lack of consensus between different gynecological scientific societies on its use [9, 10] and the several disadvantages of the Da Vinci platform [11, 12, 13] are some of the reasons why only 4%–10% of all minimally invasive surgeries are performed robotically [14, 15, 16].
The Multi-Incision approach derived from classic laparoscopy is the most commonly used approach in robotic surgery, but the quest to be less invasive inducing less trauma to the patient while still achieving the same functional and oncological outcomes, stimulated the development of Single-Incision alternatives. The trans-umbilical approach was the first option to be explored using the Da Vinci Single-Site platform, but the transvaginal route is considered the ultimate step in ultra-minimally invasive and scarless surgery.
Since laparoscopic surgery is affected by technical limitations and a long learning curve, the contribution of surgical robotic companies to the development of new surgical armamentariums is fundamental. To date, only a few companies have reached a stage of development that has granted them approval to operate in humans. The current manuscript aims to unveil the new frontier explored by these new devices based on peer-reviewed scientific publications, studying their application in gynecology.
The authors will present the results according to the following structure (Fig. 1):
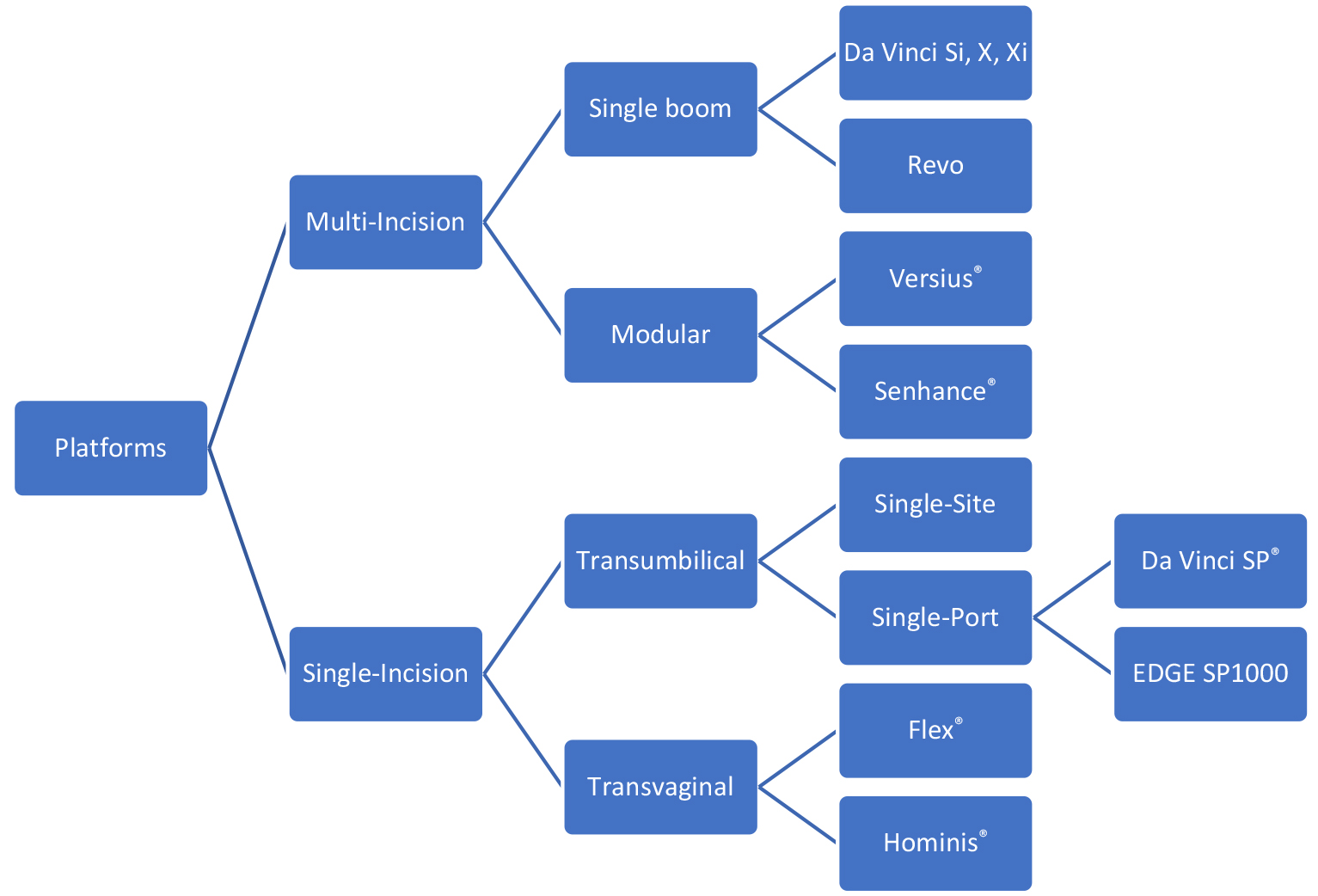 Fig. 1.
Fig. 1.Multi-Incision new robotic platforms.
Developed by Meere Company Inc. (Seongnam, Korea) its latest version was patented in 2014. After several preclinical and clinical studies, the Korean Ministry of Food and Drug Safety approved Revo-I for clinical use in 2017.
This platform has a closed console, four-arm operation carts mounted in a single boom, and a 3D high-definition (HD) vision cart [17]. The active and passive components of the arms are controlled by two manipulator operating hands. Two arms support the working instruments, a third arm manipulates the 3D HD scope, and the fourth arm uses one instrument for organ or tissue retraction. These reusable instruments are introduced through 8-mm laparoscopic trocars, have integrate motion scaling and tremor filtration, and seven degrees of motion [18, 19, 20]. Several preclinical studies have shown its potential for use in gynecological surgeries, but no clinical studies have reported its use in this surgical specialty [18, 19, 21]. The performance of cholecystectomies [21], radical prostatectomies [22, 23], and pancreatectomies [24] evidenced a short learning curve on its use [18], convenient console and video monitor, comfortable docking, outstanding camera resolution, few “foggy effects” of cautery, and effective articulated instruments [20, 22, 24].
These studies also revealed several disadvantages, namely, the need to carefully dock the robotic arms to avoid external and/or internal collisions, occasional interruptions of the surgical flow due to safety alarms, lack of sensitivity in the recognition of instruments, scissors not sharp enough, limitations in the needle driver’s range of motion, and limited diversity of robotic instruments, particularly because only monopolar and bipolar energy devices were available [21].
The fact that no retail price was reported and that the robotic system and instruments used in those studies were internally funded precluded any conclusion on the cost-effectiveness of its use, although it is presumably less expensive due to the reusability of its surgical instruments.
Developed by CMR Surgical, Inc. (Cambridge, UK), the Versius® robotic system has the goal of improving communication, ergonomics, size, and mobility in robotic surgery. Using end-user feedback in all steps of its development, an open console was built to enable easier communication between surgical team members and to facilitate training and teaching.
The open console was built to allow the surgeon to stand or sit with armrests while operating. The wheeled, 3–5 compact and mobile bedside units support the arms and have maximum flexibility to fit inside a standard size operating room (OR) and allow movement within or between ORs [25]. The console display has 3D HD video images, and the surgeon’s display shows the active instruments, system warnings, and functions. The visualization bedside unit has an auxiliary display that provides 2D HD images of the surgical field and supports the endoscope arm. The robotic handles mirror video gaming controllers, and the tips of the instruments have 7 degrees of freedom of motion.
Although preclinical studies did not contemplate any gynecological surgeries, the clinical phase of development involved the surgical treatment of several benign and malignant gynecological diseases, demonstrating the feasibility of these procedures with comparable oncological outcomes [26, 27].
A short learning curve was documented in the docking and total surgical time after the 5th surgery, easy mobilization of the console and its individual robotic arms, and the possibility of reproducing the laparoscopic port placement and laparoscopic steps of the procedure [26, 27]. The major disadvantage encountered was the limited choice of energy sources for coagulation, because only monopolar and bipolar energy were available [26, 27].
Initially developed by SOFAR Surgical Robots (Milan, Italy), it was named Telelap ALF-X and was patented in 2007. Announced as a novel robotic system in 2012, it was approved by European regulators for clinical use in gynecology, urology, general, and thoracic surgery in 2014 [28]. It was acquired by TransEnterix Surgical Inc. (Morrisville, NC, USA), renamed Senhance®, and the FDA approved its use in cholecystectomies and inguinal hernia repairs in 2017 [29].
It has an open console, 3D HD vision with up to 6x magnification, requires polarized glasses, and incorporates an eye tracking system to control camera movements. Similar to laparoscopic handpieces, two handles manipulate three independent robotic arms mounted on separate carts [30]. The 3- and 5-mm robotic instruments are fully reusable, have up to six degrees of freedom of movement, and transmit haptic feedback [27, 31].
In dry and wet laboratory settings, no gynecological surgeries have been simulated using ovine or porcine models [31, 32]. Clinical studies have been performed in several countries and different surgical specialties [33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44, 45, 46, 47, 48, 49, 50, 51, 52, 53]. Its feasibility, safety, and effectiveness of use in the surgical treatment of different benign and malignant Gynecological diseases was studied, reporting good results [34, 45, 47, 48, 54].
Senhance® was found to be a suitable alternative when compared to laparoscopy [55] and the use of 3- and 5-mm robotic instruments allowed the surgeon to follow the standard setup of mini-laparoscopy. The authors reported that the haptic feedback was reliable [36, 49, 56, 57, 58], the eye tracking feature allowed efficient management of the visual surgical area [36, 56, 57, 58] and the independent arms allowed the use of the classic laparoscopic configuration [31, 33, 39, 44, 49]. Studies in obese patients showed neither limitations in the movement of the instruments around the fulcrum nor any distortion of tactile feedback [52].
However, the need to develop wristed needle holders, articulated hooks, and new ultrasonic and stapling devices became relevant [46, 59, 60, 61]. The eye-tracking feature requires calibration before each surgical session and requires adaptation to its use [36, 56, 57, 58]. The major limitation was related to the large footprint of the arm booms in the operating and storage rooms [31, 33, 39, 44].
A dry laboratory training program for skill acquisition and surgical technique refinement, and a clinical “integration program” contemplating a 4-day internship and proctored evaluation during the transition period to the clinical practice were developed [53, 62, 63]. Cost analysis studies have also been reported, showing low-cost consumption of robotic materials, with lower median cost when compared to the Da Vinci platform, and comparable cost to laparoscopy [64, 65].
The SS was developed in 2010 and used the Si platform and a set of special accessories that included a 4-lumen port, two SS semi-rigid instruments, two straight cannulas, one 8.5-mm 3D HD endoscope, one 5/10-mm accessory port, and one insufflation valve.
The SP® was approved by the FDA in 2019 for urologic and transoral otolaryngology procedures [63], using either the Si, X, or Xi platforms, and having a single instrument arm with four instrument drive units. Through a 25 mm SP® multichannel port, the surgeon can control a 10-mm EndoWrist camera with 12 lives, wristed monopolar curved scissors, Maryland bipolar forceps, fenestrated bipolar forceps, needle driver, and Cadiére forceps. Their elbow joints allow the maintenance of intracorporeal triangulation, and the instrument guidance system displays the instrument locations inside the operative field [66, 67].
Preclinical studies have used the SS platform to perform a variety of gynecological surgeries in porcine and cadaveric models using an umbilical approach [68]. The clinical studies showed the feasibility, safety, and effectiveness of the SS and SP® platforms in the performance of a wider variety of benign and malignant gynecological procedures, enrolling an increasing number of patients [69, 70, 71, 72, 73, 74, 75, 76, 77, 78].
The introduction of bipolar instruments [71], wristed needle drivers [79], and SS ports able to accommodate the SP® cannula, and three other laparoscopic instruments at the same time represented improvements [78]. Important studies comparing SS against Multi-port and SS against SP® showed less post-operative pain, comparable surgical outcomes, shorter postoperative hospital discharge, cost reduction in surgical instruments, total hospitalization cost, and higher patient satisfaction [80, 81, 82].
EDGE Medical Robots (Shenzhen, China) developed the EDGE SP1000 with a surgeon console, patient cart, and 3D HD vision cart. The surgeon console has two control handles, a foot switch, multiple foot pedals, and two master manipulators. It integrates three wrist-type manipulator arms and a flexible camera manipulator arm [83]. The description of its structure and the only published preclinical study using a porcine model to perform an SP total hysterectomy lacks detailed information, although its features seem quite similar to the Da Vinci SP® platform [83].
Medrobotics (Raynham, MA, USA) blended laparoscopic, robotic, and colonoscopic technologies to develop a single-port operator-controlled flexible robotic system. Already approved by the FDA for colorectal procedures, the Flex® Robotic System can be docked using the Flex® Colorectal Drive, utilizing a reusable access channel. Through a transvaginal approach, the camera and working head can navigate to the target anatomy with adequate triangulation and purposeful steering of the instrument head, along with nonlinear, circuitous lumens and anatomical pathways to access the surgical field [84].
The device was tested in a preclinical setting to perform robotic transvaginal hysterectomy and salpingo-oophorectomy in cadaveric and ex vivo models. Although the need for laparoscopic assistance for tissue retraction and the lack of a flexible robotic vessel sealer or clip applier to manage the arterial vessels still need to be addressed, this device is not far from being the ideal technology to perform a robotic vaginal access minimally invasive surgery (RVAMIS) [85].
Memic Innovative Surgery Ltd. (Or Yehuda, Israel) developed an easy-to-handle
lightweight (
The two handles are Joysticks that control the arm movements corresponding to the respective hands of the surgeon. These arms include rigid and flexible sections and are inserted transvaginally through the posterior fornix into the pelvic cavity. Its flexible section functions as an instrument that can rotate and flex. The distal ends of the effector enable grasping, blunt dissection, approximation, and electrosurgery. Dependent on the classic laparoscopic view, these articulated flexible robotic arms allow the surgeon to reach various structures in the pelvic and abdominal cavities [86].
This platform was specifically designed to facilitate single-incision robotic vaginal natural orifice transluminal endoscopic surgery (RvNOTES), and two prospective clinical studies have reported the performance of eight bilateral salpingo-oophorectomies [87] and 30 hysterectomies [88] to treat benign diseases, with good intra-, peri-, and post-operative outcomes. A rapid learning curve was observed and no device-related adverse events were reported, proving the feasibility and user-friendliness of RvNOTES with this system.
Intuitive® is the major player in the market of robotic surgical platforms. Their surgical system solved problems that limited the evolution of minimally invasive surgery, introducing high-quality 3D HD surgical vision, favorable console ergonomics, and wristed surgical instruments while maintaining similar effectiveness in the surgical performance of the surgeons and disease cure rates [89, 90].
However, in order to perform an ultra-minimally invasive procedure, surgical techniques have shifted from multiport, multi-incision to single-incision surgery, using either a transumbilical or transvaginal approach. This evolution forced Intuitive to present new technical solutions and favored the development of other surgical robotic companies that delivered novel systems to tackle Da Vinci’s drawbacks in its maneuverability inside the OR and inside the patient. One of the newest potential contenders is Hugo™ RAS (Medtronic, Minneapolis, MN, USA), a multi-incision modular platform, that only has very few publications in the field of Urology [91, 92, 93].
In this review, we describe Multi-Incision and Single-Incisionrobotic platforms. The former group encompasses Single-Boom platforms, which include Da Vinci Si, X, Xi, and Revo-I, and Modular platforms that include the innovative Versius® and Senhance®. In the latter group, we found systems that used either the Transumbilical approach, such as Da Vinci SS, Da Vinci SP®, and EDGE SP1000, or the Transvaginal approach, such as the Flex® and Hominis® robotic systems (Fig. 1).
Several advantages were identified in the new multi-incision robotic platform group. Revo-I introduced haptic feedback to improve tactile recognition of anatomical structures and presented instruments with an increased lifespan that will lower the price per patient of robotic surgery, although the life-span range is not specified in the published articles.
Versius® introduced the concept of collaborative surgery, allowing two surgeons to operate at the same time in two different surgical fields, without the need to redock; an open console, which enables easier communication between the surgical team, facilitates training and teaching; independent arms, with a small footprint and with great mobility within or between ORs; ergonomic handgrips, console without pedals, and surgeon’s seat with arm rests, directly improving ergonomics and potentially increasing the surgeon’s career longevity; surgical instruments with a life span of 20 lives; and the possibility of mirroring classic laparoscopic trocar placement.
Senhance® has an open-console, modular arms, and introduces new features, namely an eye-tracking control system, to allow the surgeon to better control the visualization of the surgical field; haptic feedback that theoretically might improve recognition of anatomical structures; 3- and 5-mm reusable and wristed instruments and trocars, which are important for performing a mini-laparoscopic approach and potentially decrease the price per patient of robotic surgery.
In the group of novel Single-Incision robotic platforms there are systems that use a transumbilical or transvaginal approach. Inside the former subgroup, we have Da Vinci SS which presents a new port device kit that allows the performance of SS surgery through a transumbilical approach using the Si platform. Being a feasible and safe approach for all gynecological surgical procedures, a recent systematic review showed no significant differences in operative time, estimated blood loss and hospital stay in either benign or malignant conditions [94].
Da Vinci SP® introduced several important innovations to perform an ultra-minimally invasive procedure. It has a single arm attached to the patient cart, with four instrument drives, a small 25 mm SP® multichannel port, a camera with 12 lives, articulated in order to prevent instrument collision and optimize visualization; its instruments have elbowed joints, are fully wristed, allow intracorporeal triangulation, have 20 to 25 lives, and offer enough variety.
EDGE SP1000 features are poorly described in the very few published articles, and include a 25 mm trocar, a mounting sleeve, and articulated robotic instruments similar to the Da Vinci SP® platform.
The other subgroup of single-incision platforms uses a transvaginal approach. By blending colonoscopic, laparoscopic and robotic technology, Flex® does not present a “formal” console, neither “formal” arms, and introduces innovative fully flexible instruments.
Hominis® was specifically developed for the transvaginal approach, and presents innovative solutions. It has an open Control console where the surgeon can seat comfortably and use it as the main Human Machine Interface. The rigid part of the Hominis® Arms is inserted transvaginally, and its fully flexible part corresponds to real surgical instruments.
The preclinical development of different systems has been reported in different settings. Senhance® reported its initial development in a dry laboratory [28, 59, 62, 63], Revo-I and Senhance® performed preclinical studies using porcine models [18, 21, 50, 95, 96], Versius® was developed using porcine and cadaveric models [97, 98, 99, 100, 101, 102, 103, 104], EDGE SP1000 reported one study done in a porcine model [83], Flex® used cadaveric and ex vivo models [85]; EDGE and Hominis® did not report any information on this topic.
In all clinical studies performed with Da Vinci SS [72, 73, 74, 76, 77, 78, 105, 106, 107, 108, 109, 110, 111], Versius® and Senhance® initially treated benign gynecological diseases and progressively treated pre-malignant [26, 33, 34, 45, 46, 48, 54, 55, 60, 112], and malignant diseases from the moment they felt comfortable with its use [31, 33, 45, 54, 61]. In addition, for the development of Hominis®, several gynecological surgeries were performed to treat non-malignant diseases [87, 88], and EDGE and Flex® did not report any clinical studies.
Revo-I clinical studies have been performed exclusively in the Republic of Kore [18]. Versius® reports studies done in the UK [26, 113]. Senhance® has publications from centers in Italy, U.S, Lithuania, Germany, Japan, France, and Croatia [33, 34, 43, 45, 48, 54, 60, 64, 112]. Da Vinci SS and SP® have clinical publications from various centers in different countries. Hominis® reported one clinical study gathering data from two centers in two different countries, and no clinical data were described for EDGE and Flex®.
The authors also found common problems in all studies. No retail price of robotic systems or their instruments has been reported. No multi-center, retrospective, randomized controlled trials or matched-case analysis studies were found, and all included a small number of cases with short-term or no follow-up.
In spite all the advantages and advances these platforms still present limitations.
Revo-I had arms that sometimes were not sensitive enough to recognize the inserted instruments; its scissors lost their sharpness after few utilizations, the needle driver was pointed to have a limited range of motion, and there was limited diversity of energy devices because only monopolar and bipolar energy were available.
The main limitation of Versius® was found in the sources of energy for coagulation, as only monopolar and bipolar energy were available.
Senhance® also presented a limited variety of advanced energy instruments and no robotic stapling devices. Although the new eye-tracking feature was efficient in his task, it required calibration before each surgical session and adaptation to its use. The main issue with this platform was the large footprint of its modular robotic arms inside the OR and the storage room.
Da Vinci SS was Intuitive’s first robotic version for the SS approach and therefore presented several insufficiencies, namely, the hardware and software of the Si Surgeon console and Patient Cart were not completely adequate for single-incision surgery; the camera was not articulated, and it was difficult to achieve triangulation because the SS port had curved cannulas and the instruments were semi-flexible and not wristed.
Flex® has the potential to be the future of ultra-minimally invasive scarless surgery but still requires laparoscopic retraction to guarantee control of the surgical field, and it does not have a flexible robotic sealer or clip applier, which are important tools before transitioning to clinical trials.
Hominis® still requires a laparoscopic view, which might be solved with the introduction of an articulated robotic camera.
The acquisition price of the platform and its surgical instruments determine the cost per patient and procedure, which limits the wider dissemination of robot-assisted surgery [114]. Based on the use of the Da Vinci platform, data suggest that the cost of robotic gynecologic surgery decreases with procedural volume [115]. This cost reduction is more pronounced in endometrial cancer, more modest when performed for benign diseases [116], although Da Vinci-assisted hysterectomy still remains substantially more costly than laparoscopic hysterectomy [117, 118].
Some comparative studies between the Single-Site and Multiport systems
demonstrate a total cost decrease of approximately $2591 per patient with the
use of the former, owing to the lower cost of disposable robotic single-site
equipment [119]. It was shown that the cost per patient of the
Senhance® platform could be 2
Studies comparing Single-Site vs. Multiport and Single-Site vs. Single-Port concluded that although all of them were effective and safe in the performance of different surgeries, SP® seemed to be the best option because it is less invasive and achieves shorter docking and cervix suturing times. Unfortunately, no study has compared different platforms from competitor companies.
Training is a major concern and a priority when introducing a novel robotic platform [121, 122, 123]. In this field, CMR describes the effectiveness of a 3.5 day training program for new users, independent of their laparoscopic or robotic experience [113, 124]. Senhance® focused on the need for skill acquisition, refinement of surgical robotic techniques, and the learning curve of surgeons. In spite of the rapid adaptation to the platform regardless of their experience level, and of the rapid learning curve among experienced surgeons [62, 63], an internship clinical integration program for the surgical team with theoretical and practical courses, dry and wet laboratory training and proctoring during the first clinical cases, was developed for Senhance® [31, 53].
The authors point out that Da Vinci SS uses Si, X, and Xi platforms that have shown good surgical outcomes in minimally invasive gynecological clinical practice. Da Vinci SP® introduced the real innovative concept of single-port surgery, opening the field of ultra-minimally invasive surgery, by presenting a patient cart with a single arm and four instrument drives. Although Revo-I and EDGE SP1000 showed interesting preliminary data, they can be considered less innovative and seem to have features already present in the previous Da Vinci platforms. Versius® and Senhance® introduced a new concept of an open surgeon console and modular robotic arms. Flex® and Hominis® still need solid clinical studies to prove their clinical value, but they were able to introduce disruptive technology that will probably allow the gynecological surgical community to safely and effectively perform ultra-minimally invasive and scarless robotic surgeries in different anatomical fields (Fig. 2).
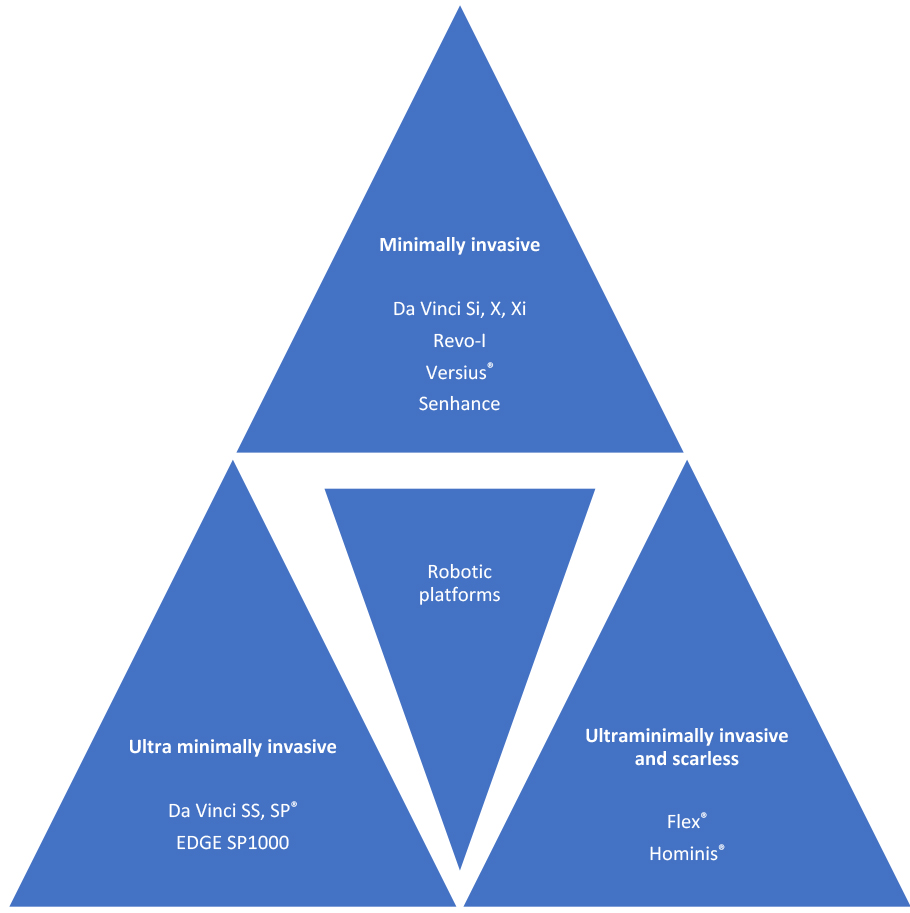 Fig. 2.
Fig. 2.Final remarks.
Da Vinci Si, X, and Xi allow safe and effective performance of small multi-incision robot-assisted laparoscopic gynecological surgery, but surgical innovation has tackled some of its drawbacks through the introduction of Revo-I, Versius®, and Senhance® robotic platforms. The development of Da Vinci Single-Site and Single-Port achieved less invasiveness through the use of a single-site transumbilical incision. Nevertheless, the innovative technology introduced by Flex® and Hominis® robotic systems may allow gynecological surgeons to achieve the golden goal of ultra-minimally invasive scarless surgery.
Study conception and design—RF, LS, CAB, SY, SP, PK, AleM; Acquisition of data—RF, LS, MP, CAB, AngM, AP, LN, TC, SA, MCS, SY, PK, ST, FF, GG; Writing – original draft—RF, LS; Writing – review & editing—RF, LS, MP, SP, RDG, GDN, GG, BR, AleM. All authors read and approved the final manuscript.
Not applicable.
Not applicable.
This research received no external funding.
The authors declare no conflict of interest. GG is serving as one of the Guest editors of this journal. We declare that GG had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to JO.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.