

Clinical and Experimental Obstetrics & Gynecology (CEOG) is published by IMR Press from Volume 47 Issue 1 (2020). Previous articles were published by another publisher on a subscription basis, and they are hosted by IMR Press on imrpress.com as a courtesy and upon agreement with S.O.G.

1 Clinical Science Department, College of Medicine, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Abstract
Purpose of Investigation: Spontaneous bilateral tubal ectopic pregnancy (BTP) is the rarest form of ectopic pregnancy. Materials and Methods: A case of BTP diagnosed during surgery is reported and an algorithm has been proposed for the management of such patients. It is a case of a 32-year-old female at gestational age of nine weeks with spontaneous pregnancy reported vaginal bleeding. Results: The case describes the importance of identifying and examining both tubes at laparoscopy, despite the rarity of bilateral extra-uterine pregnancy. Emergency exploratory laparotomy revealed ruptured ectopic pregnancy along with active bleeding of the right tube (fimbrial region). The left tube was distended with a 3×4-cm mass at the fimbrial region. Conclusion: Bilateral conservative surgery is possible with unruptured ectopic tubal pregnancy.
Keywords
- Bilateral ectopic pregnancy
- Bilateral extra-uterine pregnancy
- Contralateral salpingestomy
- Exploratory laparotomy
- Misdiagnosis
- Unilateral salpingectomy
Spontaneous bilateral tubal pregnancies (BTP) without previous induction of ovulation are considered to be unusual. The incidence of BTP has been reported from one in 725 to one in 1,580 ectopic pregnancies, one per 200,000 in normal pregnancies (live births), and five in one million deliveries [1-3]. BTP is considered to be the rarest form of ectopic pregnancy, which occurs spontaneously [1]. The diagnosis of BTP is critical because it is associated with morbidity and mortality. Most of the patients with BTPs have similar symptoms, signs, and risk factors to those with unilateral ectopic pregnancy. The main risk factors for ectopic pregnancy include multi-sexual partner, history of reproductive system infection, induced conception cycle, history of infertility, cigarette smoking, and intra-uterine device usage [4].
According to the World Health Organization (WHO), 5% of maternal mortality is due to ectopic pregnancy in the developed countries. Hemorrhage and infection cause 50% of the deaths, associated with ectopic pregnancy [5]. There has been an increase in the number of published case reports of BTPs following the use of induction ovulation, but spontaneous BTP remains a rare event [1, 6]. Recurrent ectopic pregnancies occur in 6-16% of women with a previous history of ectopic pregnancy. It has been observed that many women, for unknown reasons, failed to conceive even after successful reconstructive tubal surgery; therefore, counselling is very important. This study reports a 32-year-old female (gravida 6, para 4+1) with spontaneous BTP, who underwent exploratory laparotomy.
A 32-year-old female (gravida 6, para 4+1) at gestational age of nine weeks with spontaneous pregnancy presented to the emergency room with complains of lower abdominal pain and spotting of seven days. There was no history of fever, vomiting, change of bowel motion or urinary symptoms. She has four children, who were born at full term of gestation with normal spontaneous deliveries and she also had one abortion. The patient underwent para-umbilical hernia repair seven years prior.
General examination revealed that her pulse rate was 95 beats/minute, blood pressure was 100/60, and temperature was 37°C. The patient did not seem pale and her abdomen was tender on palpation. The pelvic examination revealed that there was mild vaginal bleeding. The uterus was bulky and both adnexa were tender on palpation, while cervical excitation was also present.
Hematological evaluation showed white blood cell count of 16, haemoglobin 11 gm/dl, hematocrit 33%, and ß-hCG was 4,900 IU/L. Transvaginal ultrasound revealed empty uterine cavity, a 30×20-mm left adnexal mass suggestive of ectopic pregnancy, and moderate amount of blood was seen in pouch of Douglas. Exploratory laparotomy was performed because of acute abdominal pain and report of blood in the pelvis.
The patient was counselled regarding the possibility of an ectopic pregnancy, and informed consent was taken for exploratory laparotomy with the possible need for performing salpingectomy or salpingostomy. Emergency exploratory laparotomy revealed ruptured ectopic pregnancy with active bleeding of the right tube (fimbrial region). The left tube was distended with a 3×4-cm mass at the fimbrial region. Fresh blood was dripping from the fimbrial end of the left tube, and hemoperitoneum was approximately 1,000 ml. In order to overcome these complications, the following procedures were performed: right salpingectomy, milking of the left tube, cauterization of the bleeding spot of the left tube, and suction and irrigation of the pelvis
The products extracted from the left tube and cut portion of the right tube with ectopic pregnancy were sent for histopathological examination. The examination showed presence of chorionic villi on both sides, which confirmed the diagnosis of bilateral ectopic pregnancy. The postoperative course was uneventful and the patient was discharged three days after the operation. The serum ß- hCG levels were declined to an undetectable level during 14 days.
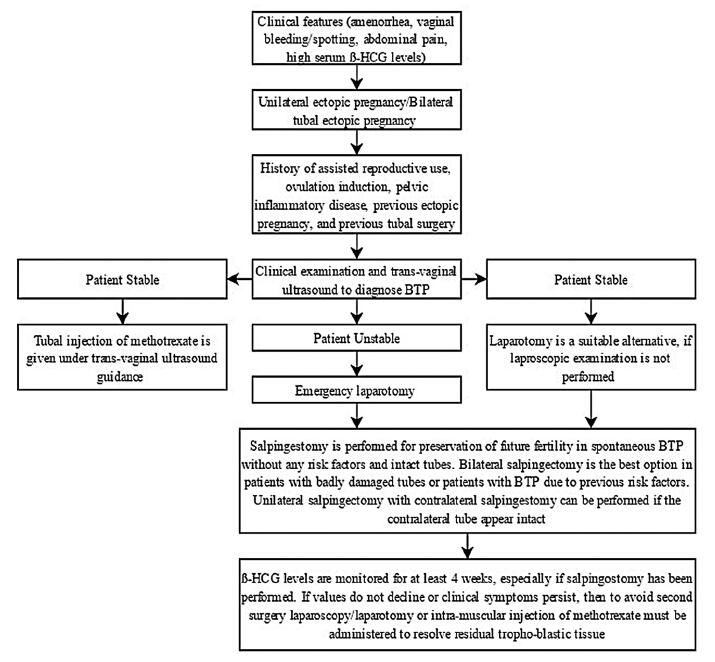 Figure 1.
Figure 1.— Algorithm for the management of suspected bilateral tubal ectopic pregnancy.
Most of the BTP cases are a result of assisted reproductive techniques (ARTs) [7]. It can also be witnessed in normal menstrual cycles. The mechanisms of BTP include multiple ovulation and trans-peritoneal migration of trophoblastic tissue from one tube to another, or superfetation [8]. The diagnosis of BTP is rarely confirmed before surgery as the clinical presentation of BTP is non-specific. There are no unique clinical features to differentiate it from unilateral ectopic pregnancy. Particularly for non-simultaneous BTP, the diagnosis of BTP is critical on the basis of serum β-HCG levels and transvaginal ultrasound scan.
The criteria for diagnosis of BTP was first suggested by Fishback and later revised by Pezzani [9, 10]. It stated that microscopic demonstration of chorionic villi in each tube was sufficient for the diagnosis of BTP. The diagnosis of BTP is usually performed intraoperatively; therefore, identification and examination of both tubes at the time of surgery is necessary [11]. The management of this condition varies, depending upon the condition of the patient, extent of tubal damage, and the desire for future fertility [1].
Medical management of BTP diagnosed preoperatively is done by injecting methotrexate into each tube under the guidance of transvaginal ultrasound [12]. It is essential to diagnose BTP accurately because failure of medical management with administration of methotrexate later becomes BTP [13]. Intramuscular injection of methotrexate in a dose of 50 mg/m2 has also been used to resolve persistent ectopic pregnancy after laparoscopic bilateral salpingostomy [12]. There are no case reports of successful primary medical treatment with methotrexate, since the diagnosis of BTP is usually made at the time of surgery.
Surgical management of BTP include salpingectomy, linear salpingostomy, bilateral salpingostomy, and bilateral salpingectomy [3]. The procedure of laparoscopy is the best option for diagnosis and management of BTP [14]. However, there is a need to maintain a high index of suspicion for BTP as the diagnosis can also be missed on laparoscopy [14]. Laparotomy is equally effective for hemo-dynamically unstable patients. Serial β-hCG monitoring should be done as there is a high risk of persistent ectopic pregnancy, especially when the patient has undergone conservative surgery (salpingostomy) or milking of the tube has been performed [1]. The reports of intra-uterine pregnancy exist after conservative surgical management of BTP, but the patients were at high risk for recurrent ectopic pregnancies in the future [1, 3, 15]. A simple management algorithm has been proposed for women with possible BTP to minimize the possibility of missing or misdiagnosing BTP [16] (Figure 1).
BTP is more often seen among the patients undergoing ARTs. However, it is important to be aware that this rare and potentially fatal condition can also occur in patients, who do not represent any risk factors of BTP. Surgeons should always keep the possibility of BTP in mind. An attentive examination of the pelvis, especially the two fallopian tubes, is necessary for early diagnosis of BTP. During conservative surgery of the fallopian tube, the main focus is towards the prevention of tubal damage. After an incidental finding of unilateral or bilateral ectopic pregnancy, appropriate surgical procedures must be considered in the patients. The choice of fertility preserving surgery must be weighed against the increased risk of recurrence.
The author is very thankful to all the associated personnel of any reference that contributed in/for the purpose of this research.