
Academic Editor: Alpo Vuorio
Background: The coronavirus disease-2019 (COVID-19) pandemic is surging
across Poland, leading to many direct deaths and underestimated collateral
damage. We aimed to compare the influence of the COVID-19 pandemic on hospital
admissions and in-hospital mortality in larger vs. smaller cardiology departments
(i.e., with
The coronavirus disease-2019 (COVID-19) pandemic has affected more than 458 million people worldwide. In Poland, the total number of infected patients has reached more than 6 million people accounting for more than 15% of Polish population [1]. There were more than 116 thousand COVID-19 deaths with mortality rate of about 1.9%. The COVID-19 pandemic has become the most challenging public healthcare emergency of our times. Limited availability of specialist care together with omnipresent fear of getting infected with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) have contributed to reduction in hospital admissions due to acute cardiovascular conditions [2, 3, 4, 5, 6, 7, 8]. From the Polish perspective, there were reports of decline in-hospital admissions due to various cardiovascular emergencies, together with reduced number of coronary angiographies, percutaneous coronary interventions, both transthoracic and transesophageal echocardiographic examinations, as well as electrotherapy and electrophysiology procedures [9, 10, 11, 12, 13, 14, 15, 16]. Postponing the seek for medical attention due to various cardiovascular emergencies, such as acute coronary syndrome or acute heart failure (AHF), is associated with worse prognosis or can lead to death [17, 18, 19, 20]. Patients with AHF require urgent in-hospital diagnostics and treatment, while those presenting with more advanced symptoms (higher New York Heart Failure [NYHA] class) have worse prognosis [21]. Clinical presentation of AHF and COVID-19 includes acute dyspnea, bringing another diagnostic challenge. Yet, the co-occurrence of AHF and COVID-19 is associated with high mortality [22, 23, 24, 25].
In our recently published Impact of COVID-19 pandemic on acute Heart Failure admissions and mortality: multicentre COV-HF-SIRIO 6 study, we have found that the COVID-19 pandemic has led to reduced hospital admissions for AHF with a significantly lower number of self-referred AHF patients and a higher number of AHF patients brought by an ambulance [26]. Furthermore, the mortality rate for AHF during the COVID-19 era was significantly increased, particularly for concomitant AHF and COVID-19.
We performed this subanalysis of the COV-HF-SIRIO 6 study aiming to compare the influence of the COVID-19 pandemic on hospital admissions and in-hospital mortality in cardiology departments hospitalizing equal or more vs. less than 2000 patients yearly.
The COV-HF-SIRIO 6 study was a retrospective analysis of hospital records of consecutive patients hospitalized in 24 cardiology departments in Poland in 2019 and 2020 [26]. We took under investigation all patients hospitalized from January 1, 2019 to December 31, 2020 (in pre-COVID-19 vs. COVID-19 eras). In this subanalysis of the COV-HF-SIRIO 6 study, we arbitrary divided all cardiology departments into two groups based on the total number of hospitalizations in 2019 (pre-COVID 19 era), with smaller departments defined as those hospitalizing less than 2000 patients, and larger departments—2000 patients or more. We focused on patients hospitalized due to AHF (International Statistical Classification of Diseases and Related Health Problems codes for heart failure I50.x), as well as those with concomitant SARS-CoV-2 infection. The diagnosis of AHF was based on the definition provided by the 2016 European Society of Cardiology guidelines for the diagnosis and treatment of acute and chronic heart failure [27]. The COV-HF-SIRIO 6 study was conducted in accordance with the Declaration of Helsinki and was approved by the Local Ethics Committee (study approval reference number KB 353/2021).
Statistical analysis was carried out using Statistica 13.0 (TIBCO Software Inc.,
California, USA). Continuous variables were presented as means with standard
deviations. Due to non-normal distribution of the investigated data, as
demonstrated by the Shapiro-Wilk test, non-parametric tests were used for
statistical analysis. Comparisons of continuous variables between two groups were
performed with the Mann-Whitney unpaired rank sum test. Comparisons between year
2019 and 2020 were performed with the Wilcoxon signed test. Categorical variables
are presented as number and percentage and were compared using the
A total of 101,433 patients were hospitalized in 24 cardiology departments in
Poland between January 1, 2019 and December 31, 2020. The study cohort was
divided into two subgroups including 69,019 patients hospitalized in larger
cardiology departments (n = 12) and 32,414 patients hospitalized in smaller
cardiology departments (n = 12). The total number of hospitalizations was reduced
by 29.2% (p
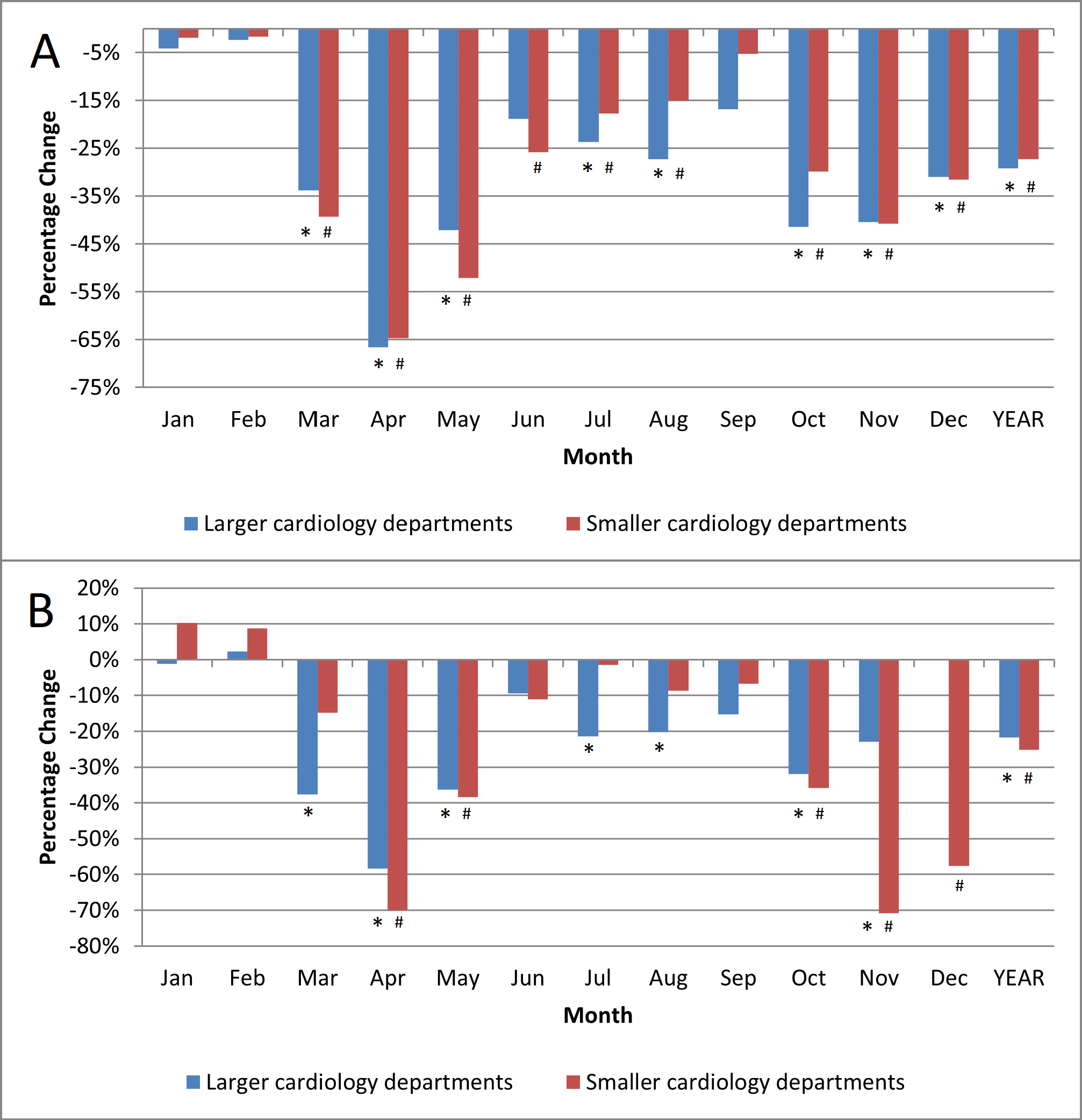 Fig. 1.
Fig. 1.Hospitalizations percentage change. (A) Reduction of all-cause hospitalizations during the COVID-19 pandemic in 2020 vs.
2019. (B) Reduction of acute heart failure hospitalizations during the COVID-19
pandemic in 2020 vs. 2019. * p
The number of patients hospitalized for AHF was reduced by 21.8% (p
Duration of hospital stay due to AHF during the COVID-19 pandemic in 2020 was
significantly longer in larger vs. smaller cardiology departments (9.6 vs. 6.6
days; p
 Fig. 2.
Fig. 2.The length of hospital stay. * p
Regardless of department size, the number of self-referrals was lower in 2020 vs. 2019, with significantly more patients brought by an ambulance (Table 1). However, this trend of decreased number of self-referrals and increased number of patients brought by an ambulance, in smaller cardiology wards visibly followed the peaks of the pandemic, having more random distribution in larger cardiology departments.
| Month | Self-reffered | Brought by an ambulance | ||||||||||||||||||
| Larger cadiology departments | Smaller cadiology departments | Larger cadiology departments | Smaller cadiology departments | |||||||||||||||||
| 2019 | 2020 | p | 2019 | 2020 | p | 2019 | 2020 | p | 2019 | 2020 | p | |||||||||
| N | % | N | % | N | % | N | % | N | % | N | % | N | % | N | % | |||||
| Jan | 131 | 45.5 | 150 | 50.5 | 0.22 | 261 | 62.3 | 309 | 66.9 | 0.15 | 154 | 53.5 | 145 | 48.8 | 0.26 | 111 | 26.5 | 109 | 23.6 | 0.32 |
| Feb | 136 | 50.4 | 145 | 50.7 | 0.94 | 239 | 62.9 | 280 | 67.8 | 0.15 | 134 | 49.6 | 140 | 49.0 | 0.87 | 89 | 23.4 | 106 | 25.7 | 0.46 |
| Mar | 167 | 49.4 | 86 | 42.2 | 0.10 | 241 | 61.6 | 213 | 64.0 | 0.52 | 171 | 50.6 | 117 | 57.4 | 0.12 | 117 | 29.9 | 96 | 28.8 | 0.75 |
| Apr | 148 | 51.6 | 47 | 38.8 | 0.02 | 282 | 63.9 | 69 | 51.9 | 0.01 | 139 | 48.4 | 73 | 60.3 | 0.03 | 110 | 24.9 | 51 | 38.3 | 0.003 |
| May | 150 | 51.0 | 92 | 47.9 | 0.50 | 267 | 67.4 | 163 | 66.8 | 0.87 | 138 | 46.9 | 97 | 50.5 | 0.44 | 92 | 23.2 | 65 | 26.6 | 0.86 |
| Jun | 119 | 46.9 | 97 | 41.1 | 0.20 | 241 | 63.9 | 206 | 61.5 | 0.50 | 132 | 52.0 | 124 | 52.5 | 0.90 | 98 | 26.0 | 88 | 26.3 | 0.02 |
| Jul | 161 | 55.5 | 105 | 44.9 | 0.02 | 248 | 61.7 | 252 | 63.6 | 0.57 | 126 | 43.4 | 125 | 53.4 | 0.02 | 105 | 26.1 | 89 | 22.5 | 0.23 |
| Aug | 136 | 47.6 | 95 | 45.9 | 0.72 | 257 | 64.1 | 235 | 64.2 | 0.97 | 148 | 51.7 | 111 | 53.6 | 0.68 | 105 | 26.2 | 100 | 27.3 | 0.72 |
| Sep | 131 | 51.6 | 108 | 47.8 | 0.41 | 247 | 63.7 | 244 | 67.4 | 0.28 | 120 | 47.2 | 117 | 51.8 | 0.32 | 99 | 25.5 | 90 | 24.9 | 0.84 |
| Oct | 188 | 60.6 | 104 | 49.8 | 0.01 | 321 | 68.6 | 156 | 52.0 | 121 | 39.0 | 105 | 50.2 | 0.01 | 101 | 21.6 | 117 | 39.0 | ||
| Nov | 155 | 53.4 | 106 | 47.7 | 0.20 | 263 | 66.6 | 46 | 40.0 | 132 | 45.5 | 115 | 51.8 | 0.16 | 102 | 25.8 | 44 | 38.3 | 0.009 | |
| Dec | 135 | 52.1 | 131 | 50.0 | 0.63 | 243 | 64.8 | 77 | 48.4 | 121 | 46.7 | 128 | 48.9 | 0.63 | 108 | 28.8 | 63 | 39.6 | 0.01 | |
| Year | 1757 | 51.4 | 1266 | 47.0 | 3110 | 64.3 | 2250 | 62.2 | 0.04 | 1636 | 47.8 | 1397 | 51.8 | 0.002 | 1237 | 25.6 | 1018 | 28.1 | 0.009 | |
| Statistical test used: | ||||||||||||||||||||
The total number of patients with concomitant AHF and COVID-19 was 160 (4.1% of AHF patients hospitalized in 2020) for larger vs. 79 (2.2% of AHF patients hospitalized in 2020) for smaller cardiology departments.
Additional beds dedicated for patients with COVID-19 were created in the majority of hospitals, however smaller departments provided more extra beds to treat COVID-19 patients as compared with larger cardiology departments (675 vs. 481 beds) (Fig. 3).
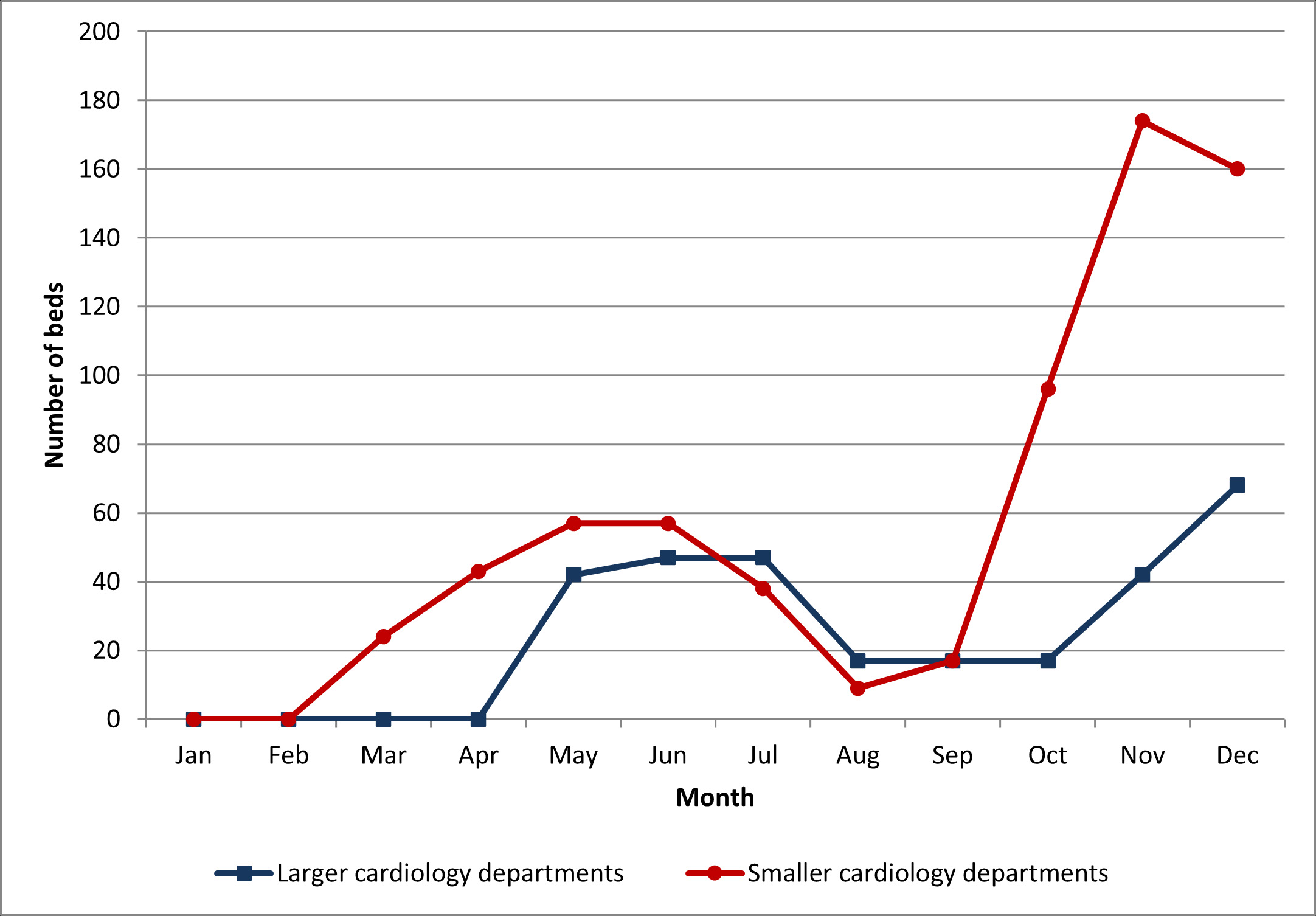 Fig. 3.
Fig. 3.Number of beds dedicated for COVID-19 patients in 2020.
In-hospital mortality rate for AHF was significantly higher during the COVID-19 era vs. pre-COVID-19 era, amounting to 10.7% vs. 8.1% (p = 0.0004) in larger cardiology departments. The mortality peaks closely followed peaks of the pandemic, with the maximum value of 18.1% in the very peak of the pandemic in November 2020 (Fig. 4).
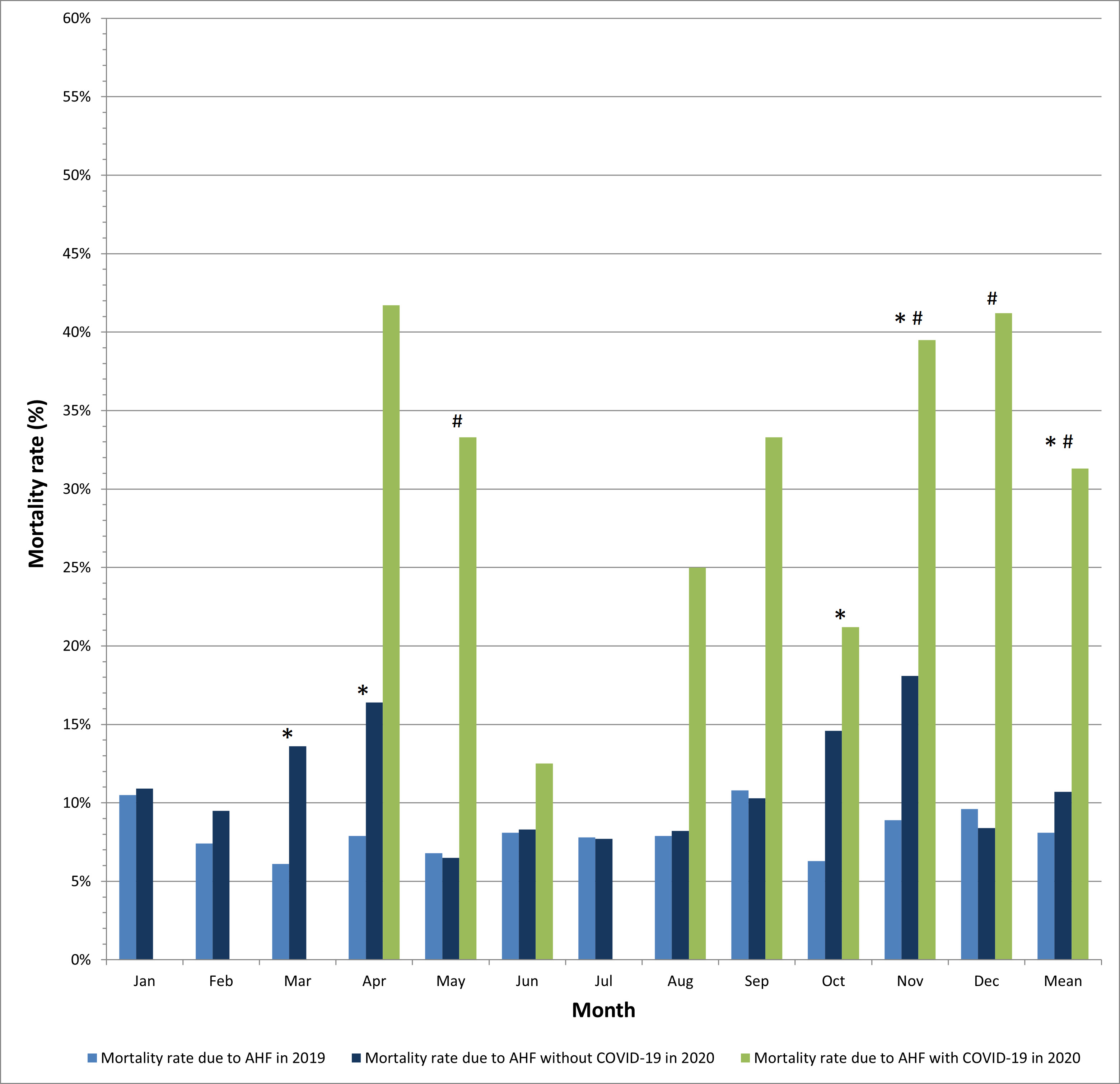 Fig. 4.
Fig. 4.In-hospital mortality due to acute heart failure in patients
with and without COVID-19 in larger cardiology departments. * p
Interestingly, the mortality rate for AHF in smaller cardiology departments did not differ significantly in COVID-19 vs. pre-COVID-19 eras (3.2% vs. 2.9%, p = 0.47) (Fig. 5).
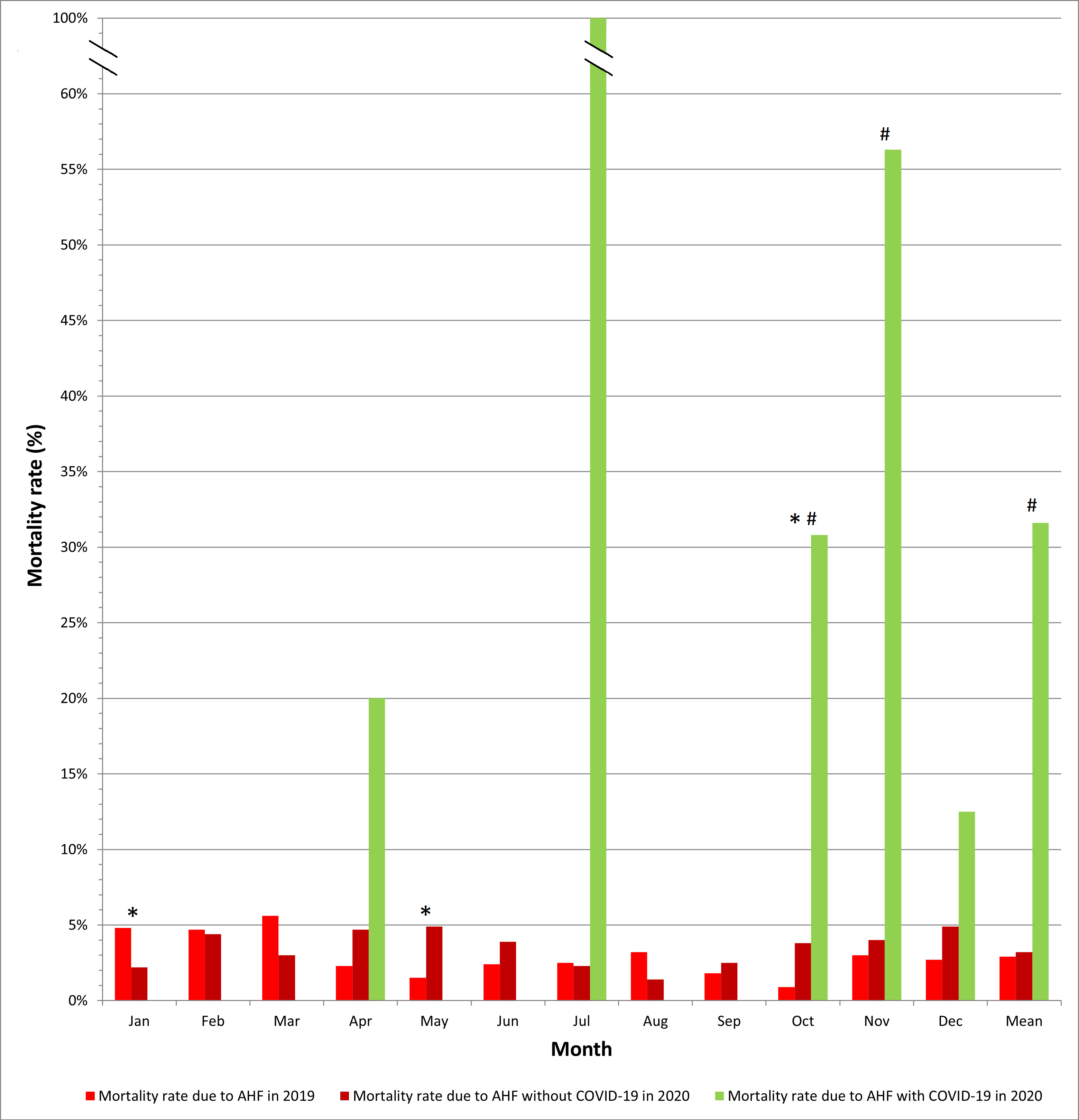 Fig. 5.
Fig. 5.In-hospital mortality due to acute heart failure in patients
with and without COVID-19 in smaller cardiology departments. * p
In-hospital mortality for AHF during the COVID-19 pandemic was substantially
higher in larger vs. smaller cardiology departments (10.7% vs. 3.2%; p
| Month | Mortality rate in AHF patients without COVID-19 | Mortality rate in AHF patients with concomitant COVID-19 | ||||||||
| Larger cardiology departments | Smaller cardiology departments | p | Larger cardiology departments | Smaller cardiology departments | p | |||||
| N | % | N | % | N | % | N | % | |||
| Jan | 35 | 10.9 | 10 | 2.2 | 0 | 0 | 0 | 0 | N/A | |
| Feb | 29 | 9.5 | 18 | 4.4 | 0.006 | 0 | 0 | 0 | 0 | N/A |
| Mar | 30 | 13.6 | 10 | 3.0 | 0 | 0 | 0 | 0 | N/A | |
| Apr | 20 | 16.4 | 6 | 4.7 | 0.002 | 5 | 41.7 | 1 | 20.0 | 0.60 |
| May | 13 | 6.5 | 12 | 4.9 | 0.46 | 3 | 33.3 | 0 | 0 | N/A |
| Jun | 21 | 8.3 | 13 | 3.9 | 0.01 | 1 | 12.5 | 0 | 0 | N/A |
| Jul | 19 | 7.7 | 9 | 2.3 | 0.001 | 0 | 0 | 1 | 100 | N/A |
| Aug | 18 | 8.2 | 5 | 1.4 | 1 | 25.0 | 0 | 0 | N/A | |
| Sep | 24 | 10.3 | 9 | 2.5 | 2 | 33.3 | 0 | 0 | N/A | |
| Oct | 29 | 14.6 | 10 | 3.8 | 7 | 21.2 | 12 | 30.8 | 0.36 | |
| Nov | 35 | 18.1 | 4 | 4.0 | 17 | 39.5 | 9 | 56.3 | 0.25 | |
| Dec | 20 | 8.4 | 7 | 4.9 | 0.20 | 14 | 41.2 | 2 | 12.5 | 0.09 |
| Year | 293 | 10.7 | 113 | 3.2 | 50 | 31.3 | 25 | 31.6 | 0.95 | |
| Abbreviations: AHF, acute heart failure; N/A, not applicable. Statistical test
used: | ||||||||||
In-hospital mortality rate for concomitant AHF and COVID-19 was extremely high both in larger and smaller cardiology departments, accounting for 31.3% vs. 31.6%, respectively (Table 2). In-hospital mortality was highest in the very peaks of the pandemic, reaching the highest value of 56.3% in November 2020 in smaller cardiology wards (the reported mortality rate of 100% is a single patient death, thus should be interpreted with caution).
The COVID-19 pandemic is still surging across the globe. Although we do not know
whether the pandemic is with us here to stay and if some temporary solutions
become permanent, we need to learn how to function in this new reality and
provide the best possible care for all patients. One of the first reports on
heart failure management in Polish medical centers during the COVID-19 pandemic
came from Lelonek et al. [28] showing reduced hospitalizations,
domination of teleconsultations over in-person visits and e-prescriptions
widespread use during the first three months of the COVID-19 pandemic in both
academic and non-academic centers. We went one step further and according to our
knowledge performed the largest multicentre study including more than 100,000
patients aiming to assess the influence exerted by the COVID-19 pandemic on
hospital admissions and in-hospital mortality, and the first study so far
confronting larger cardiology departments hospitalizing
Heart failure was found to be an independent risk factor for death in COVID-19
patients [29]. The reported in-hospital mortality for concomitant heart failure
and COVID-19 was extremely high, accounting for 49% in the very beginning of the
pandemic (March-May 2020) in a large cardiology center in the USA. In our study,
the highest mortality rate for co-existing AHF and COVID-19 in larger departments
was 41.7% at the beginning of the pandemic in April 2020. In a systematic review
and meta-analysis by Yonas et al. [30], in a group of 21,640 COVID-19
patients from 18 studies heart failure was associated with poor outcome (odds
ratio [OR] 2.86; 95% confidence interval [CI] 2.07–3.95; p
There are loads of data documenting increased mortality rates for concomitant AHF and COVID-19, however very few reports focus on the collateral damage of the COVID-19 pandemic. We found increased mortality rates for AHF in 2020 as compared with 2019, but only in larger cardiology departments. A single center Italian study by Colivicchi et al. [19] performed in a large volume hospital reported a 17.2% in-hospital mortality rate for AHF in the beginning of the pandemic in 2020 as compared with 6.3% in the time-matched period of 2019. Data arriving from two referral hospitals in London, UK, also documented significantly higher in-hospital mortality rates for AHF in 2020 vs. 2019 [32]. Studies confronting data from larger/academic hospitals with smaller/district cardiology wards are lacking. In the Danish nationwide cohort study presenting data of all patients hospitalized in Danish hospitals between January 1, 2019 and March 31, 2020 due to heart failure, there was no statistically significant increase in the mortality rates in the COVID-19 era vs. pre-COVID-19 times [33]. In our study, we did not find any differences in in-hospital mortality rates in smaller departments in 2020 vs. 2019. Several arguments may serve as potential explanation of the observed phenomenon of higher in-hospital mortality in larger vs. smaller cardiology departments. Firstly, cardiology departments defined as larger in our study were very often academic centers offering the highest level of reference and very often providing care for severely-ill patients transferred from smaller, non-academic (provincial, regional or district) hospitals. Secondly, patients with AHF with respiratory failure, requiring mechanical ventilation are usually directly admitted to larger cardiology centers. Thirdly, the mean length of hospital stay was longer in larger vs. smaller cardiology department which indirectly indicates that patients hospitalized in larger cardiology departments might have been more severely ill.
Our analysis on modes of hospital admissions showed an increased number of patients brought by emergency teams and a decreased number of self-referrals in 2020 vs. 2019. However, worth underlining is the fact that although in the COVID-19 era patients were more frequently brought by an ambulance than self-referred, the total number of patients brought by emergency teams was lower in 2020 than in 2019. These observations are in line with reports from the very beginning of the pandemic, presenting a decline in the number of interventions of emergency medical teams [34, 35, 36].
There are some limitations of our study, such as its retrospective character. Moreover, data included in the analysis were derived from hospital electronic databases lacking clinical characteristics of patients or results of additional work-up, thus they were unavailable for the assessment. Worth adding is, that only patients with COVID-19 requiring hospitalization were included in the analysis, thus we do not know if asymptomatic COVID-19 would also influence the prognosis in AHF patients.
In our subanalysis of the COV-HF-SIRIO 6 multicenter study comparing influence of the COVID-19 pandemic on hospital admissions and mortality rate in larger vs. smaller cardiology departments we found: (1) similarly reduced hospital admissions; (2) higher in-hospital mortality for AHF; (3) longer hospital stays for AHF; (4) similar and extremely high in-hospital mortality for concomitant AHF and COVID-19.
MO, MKa, WS, AKu, EPN and JKu designed the research study. MO, MKa, WS, KG, JKr, PA, PP, EAM, OMB, AC, AD, LG, PG, LK, AKl, MKos, MKoz, PK, TK, GM, MM, AP, JP, GS, BS, SSo, SSt, PS, AW, and PW collected study data. MO, MKa, WS, KG, JKr, PA, PP, EAM, OMB, AC, AD, LG, PG, LK, AKl, MKos, MKoz, PK, TK, GM, MM, AP, JP, GS, BS, SSo, SSt, PS, AW, and PW performed the research. AKu, EPN, JKr, SB, AB, RG, MGą, MGr, JD, MJ, PJ, JL, ML, PL, PM, JN, ATK, AT, TZ, JKa and JKu provided help and advice on study design and methodology. SB, AB, RG, MGą, MGr, JD, MJ, PJ, JL, ML, PL, PM, JN, ATK, AT, TZ, JKa and JKu supervised the research. MO, MKa and WS analyzed the data. MO wrote the first draft of the manuscript. All authors contributed to editorial changes in the manuscript. All authors read and approved the final manuscript.
The COV-HF-SIRIO 6 study was conducted in accordance with the Declaration of Helsinki and was approved by the Local Ethics Committee (study approval reference number KB 353/2021).
We would like to express our gratitude to the peer reviewers for their opinions and suggestions, and to all those who helped us with writing of this manuscript.
This research received no external funding.
The authors declare no conflict of interest. Eliano Pio Navarese is serving as one of the Editorial Board members of this journal. We declare that Eliano Pio Navarese had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to Alpo Vuorio.
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.