
These authors contributed equally to this work.
Sinus pneumatization is a continuous physiological process that occurs naturally and causes an increase in the volume of paranasal sinuses. Pneumatization is also frequently observed following extraction of teeth in the posterior maxilla. This leads to an increase in the sinus volume and height at the expense of the edentulous alveolar ridge. These changes may affect treatment planning if dental implants are indicated to replace extracted teeth. Using a novel method to align and compare two panoramic radiographs taken before and after tooth extraction, we aimed to examine post-extraction dimensional changes in the maxillary sinus and alveolar ridge by superimposition of preand post-treatment panoramic radiographs. Twenty-two pairs of panoramic radiographs were analyzed retrospectively for changes in alveolar ridge and maxillary sinus dimensions following at least 6 months from tooth extraction. Pre- and post-extraction radiographs were matched and then superimposed using a fixed reference unit. Measurements included the distance from bone-crest to sinus-floor and to sinus-roof, as well as distance from sinus-floor to sinus-roof and maxillary-sinus sagittal circumference. The mean difference between pre- and post-extraction bone-crest to the sinus-floor radiographic measurements was statistically significant ($P =$ 0.001) with a mean change of 1.2 mm. The difference between pre- to post-extraction bone-crest to sinus-roof measurements was insignificant ($P =$ 0.094) with a mean change of 0.9 mm. The distance between pre- and post-extration sinus-floor to sinus-roof was significantly increased in an average of 1 mm ($P =$ 0.001) along with an increase in sinus sagittal circumference from 993.9 $\pm $ 295.7 mm to 1096.6 $\pm$ 312.5 mm ($P <$ 0.0001). In conclusion, a moderate increase in maxillary sinus dimensions concurrent with crestal resorption may be anticipated after extraction of maxillary posterior teeth, leading to an overall decrease in alveolar bone height.
Sinus pneumatization is a continuous physiological process that occurs naturally and causes an increase in the volume of paranasal sinuses [1]. The maxillary sinus is the largest of the paranasal sinuses and the first to develop [2]. After birth, the sinus continues to pneumatize into the developing alveolar ridge [3]. Histologic examination shows that the pneumatization process occurs by osteoclastic resorption of the cortical walls of the sinus and the layering of the osteoid which is inferior to it [4].
The reasons for sinus pneumatization are not well understood. Among the factors that have been associated with this phenomenon are genetics, craniofacial configuration, and density of the maxillary bone, growth hormones and sinus surgery [5]. Other theories involve the pneumatizing drive of the mucous membrane of the middle ear for the mastoids and that of the mucous membrane of the nose for the paranasal sinuses, the positive air pressure and resorption of the spongiosa in the frontal and the maxillary bones for the paranasal sinuses and resorption of the mesoderm in the mastoid bone for the mastoid air-cell systems[6,7]. Pneumatization is also frequently observed following tooth extraction in the posterior maxilla[5,8], which is sometimes referred to as "disuse atrophy"[5,9]. This theory suggests that the decrease in functional forces to the bone following tooth loss causes a shift in the remodeling process towards bone resorption according to Wolff's law [10]. This in turn leads to an increase in the sinus volume at the expense of the edentulous alveolar ridge. Greater pneumatization has been found following molar extraction when compared to premolar extraction[4,5]. This may be due to the larger socket in the molar region which requires a longer healing time, thus allowing the sinus to pneumatize further. In extreme cases, tooth loss can induce maxillary sinus expansion, thus creating a union between the sinus floor and the crest of the remaining alveolar ridge [11]. This expansion is related to sinus height and length rather than depth [12]. However, the decrease in the vertical dimension of the edentulous ridge is, to some extent, also related to crestal bone loss. The loss in the alveolar bone height following extraction is predominantly of the buccal plate, which has been shown to be located 1.2 mm apically to its lingual counterpart [13]. Thus, these two processes (sinus expansion downwards and crestal resorption apically) result in the marked deficiency that is often observed in the edentulous posterior maxilla.
Changes in maxillary sinus dimensions following tooth extraction have been shown in several studies[5,14,15], while others have failed to report such changes. Rosen and Sarnat found an expansion of the sinus volume in 7 of 10 dogs at 6-12 months after extraction of all posterior maxillary teeth (compared to the contra-lateral side) [15]. In addition, Sharan and Madjar found that posterior maxillary tooth extraction caused an inferior (downwards) expansion of the maxillary sinus in relation to fixed anatomic structures in humans [16].
Previous studies which used panoramic radiographs or 2 pairs of radiographs for comparison, didn't take into account the possibility of differences in scales and/or mismatching which might arise from comparing two different panoramic radiographs that had some inherent proportional differences associated with the machine, the software, and the patient's position and posture. Sharan and Madjar used two panoramic radiographs, each of a different subject, to measure supero-inferior differences of the sinus floor position in dentate sites in comparison with contralateral edentulous sites and pairs of panoramic radiographs, each pair of the same subject, to measure supero-inferior differences of the sinus floor position in the same site before and after extraction. The images were aligned so that the interorbital line paralleled the framework of the computer screen [5]. Ohba et al., compared the depth of the maxillary sinus floor on panoramic radiographs between edentulous and dentate patients [8]. Panoramic radiographs of edentulous female patients and panoramic radiographs of female dentate patients were used for the sample. To measure the depth of the maxillary sinus floor, the outline of the maxillary sinus on the panoramic radiograph was traced on transparent paper. These methods could not account for the differences in scales and other distortions that may have caused mismatches in comparing two different panoramic radiographs.
Hence, the aim of the current study was to evaluate and compare maxillary sinus dimensions before and following tooth extraction, using a novel method to align and compare the two panoramic radiographs obtained before and after tooth extraction, while trying to compensate for possible mismatches in comparing the anatomical landmarks [17].
The research protocol was approved by the Ethical Committee of Rambam Health Care Campus, Haifa, Israel (approval # 0435-15-rmb). An initial database of 72 dental files of patients who underwent extraction of either the maxillary second premolar, first molar, or second molar at the Department of Periodontology between July 1996 and March 2016 were screened for potential inclusion in this retrospective study. Twenty-four patients from the initial database, who had both a pretreatment (Tb) and at least 6 months post-extraction (Tf) panoramic radiographs, were further screened for possible inclusion in the study. Finally, 22 patients $\geq $ 20 years of age, who had tooth extractions as stand-alone procedures (without concomitant flap elevation, socket preservation, guided bone regeneration, immediate implant placement or sinus perforation during tooth extraction), were included in the study (Fig.1).
 Fig. 1.
Fig. 1.Database flow chart.
Twenty-two subjects (13 females and 9 males), aged 34-77 (mean 59.82 $\pm $ 11.96 years) were included in this analysis. Two patients (9.9%) exhibited minor complications following tooth extraction: one had severe but transient post-operation pain and another patient suffered from prolonged bleeding at the day of the procedure. All measurements were performed twice by one examiner (I.L), following several training sessions which included identification of landmarks, matching of radiographs and measurements.
Matching and measurement technique: panoramic radiographs were used to measure sinus dimensions before extraction and at least 6 months after extraction. PowerPoint® software (Microsoft office 2016) was used to match the two radiographs using the following method [17]: the two images were set for transparency and then superimposed in the region of interest. Fixed reference structures, such as teeth and dental implants adjacent to the region of interest were selected for the matching procedure. Visual matching and alignment was performed by stretching or contracting the images until the reference structures were matched as accurately as possible. After matching, the radiographs were transferred into the Dimaxis Pro® measurement software (Planmeca Oy Helsinki Finland) version 4.1.6 for radiographic measurements (Fig. 2). The following measurements were performed:
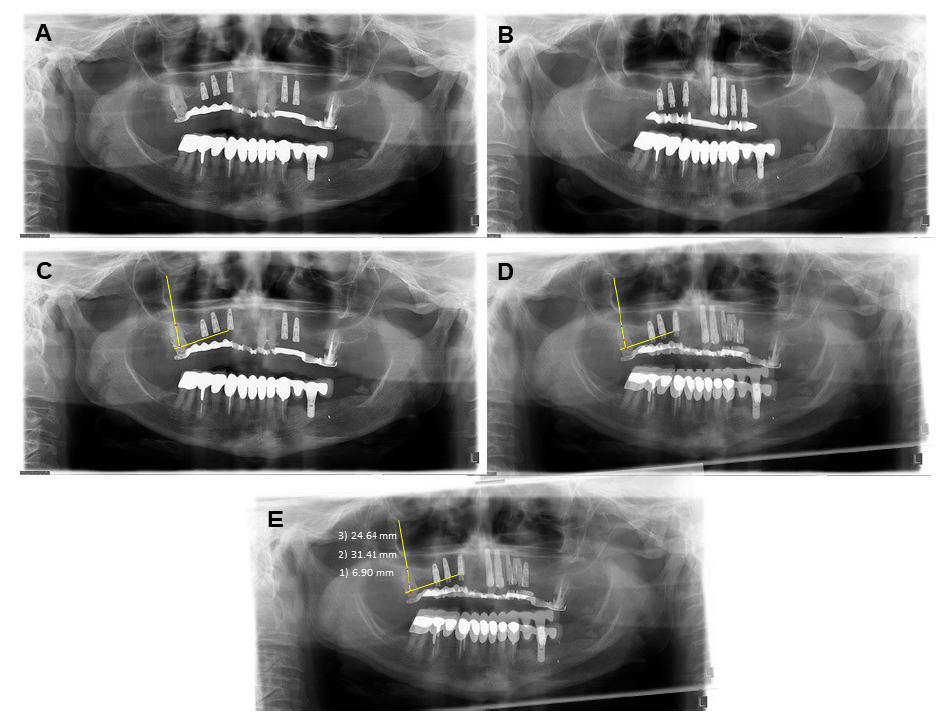 Fig. 2.
Fig. 2.Measurement technique: (A) Baseline radiograph of tooth #17. (B) Final radiograph of tooth #17, 6 months following extraction. (C) Landmark identification and definition. (D) Superimposition of the two radiographs. (E) Measurements; the distance BC-floor (1), BC-roof (2), floor-roof (3).
1. Maxillary sinus sagittal circumference -- maxillary sinus wall circumference measured on the panoramic radiograph.
2. Distance between the bone crest (BC) in the middle of the extraction site and the sinus floor.
3. Distance between the BC in the middle of the extraction site and the sinus roof.
4. Distance between the sinus floor in the middle of the extraction site and the sinus roof.
ImageJ software (ImageJ 1.50i, Wayne Rasband National Institutes of Health, USA) was used to measure maxillary sinus sagittal circumference (Fig. 3).
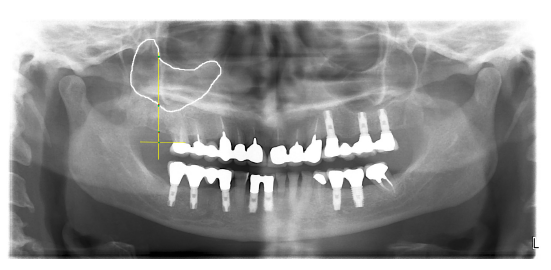 Fig. 3.
Fig. 3.Maxillary sinus sagittal circumference.
Calibration: prior to measurements, calibration was performed. A fixed reference of known dimension, such as a dental implant, which existed in both radiographs, was used as a reference point. In order to account for potential differences between radiographs, after calibration was done, an additional object which appeared in both radiographs was measured, and the difference between these two measurements was calculated (delta constant). A comparison of differences between these measurements revealed a mean difference of 0.2 $ \pm $ 0.48 mm.
Statistical analysis: data were analyzed using SPSS version 21 [IBM SPSS Statistics software (IBM Inc., Chicago, IL, USA)]. Normal distribution of the parameters was initially confirmed. Then, intra-examiner reproducibility for two sets of radiographic measurements that were performed by a single examiner was performed using a paired t-test. Descriptive statistics (mean, SD, and percentiles) were used for the categorical and quantitative parameters. Wilcoxon Signed Ranks Test was used for differences between pre- (baseline) and post-extraction in several measurements. The level of significance was set at $\alpha =$ 0.05.
A total of 22 subjects (13 females and 9 males) with a mean age of 59.8 years ($ \pm $ 11.9 SD, range: 34-77) were included in the present study. Sixteen patients (72.7%) had 20 single extraction sites and 6 patients (27.3%) had 6 multiple extraction sites (a total of 26 sites with 32 teeth). Among all extraction sites, 25% were of second premolars, 31.2% first molars and 43.8% second molars. The median follow-up period between baseline and post-extraction radiographs was 12 months (range: 6-98 months) and the mean follow up period was 25 months ($ \pm $ 26.6 SD).
The distance between the sinus floor and roof ranged from 13.5 mm to 35.9 mm pre-extraction (mean 23.6 $ \pm $ 5.4 mm SD), while post-extraction, this distance ranged from 13.3 to 37.2 mm (mean: 24.6 $ \pm $ 5.5 mm SD). These mean differences of 1.0 $ \pm $ 1.5 mm were statistically significant ($P=$ 0.001).
The distance between the BC to the sinus roof ranged from 27.1 mm to 43.7 mm pre-extraction (mean 34.2 $ \pm $ 4.4 mm SD), whereas in post-extraction this distance ranged from 20.1 mm to 44.1 mm (mean: 33.3 $ \pm $ 5.4 mm SD). The difference between pre- and post- extraction BC- sinus roof measurements was insignificant ($P=$ 0.094) with a mean delta of 0.9 mm.
The distance between the BC to the sinus floor ranged from 4.8 to 20.0 mm pre-extraction (mean 10.6 $ \pm $ 4.2 mm SD), whereas post-extraction this distance ranged from 2.6 to 17.8 mm (mean: 9.3 $ \pm $ 4.3 mm SD). These mean differences between pre and post-extraction BC to the sinus floor measurements were statistically significant ($P=$ 0.001) with a mean delta of 1.2 mm (Table 1).
| Pre floor-roof | Post floor-roof | Pre BC-roof | Post BC-roof | Pre BC-floor | Post BC-floor | |
|---|---|---|---|---|---|---|
| Teeth (n) | 32 | 32 | 32 | 32 | 32 | 32 |
| Minimum (mm) | 13.5 | 13.29 | 27.1 | 20.13 | 4.80 | 2.64 |
| Maximum (mm) | 35.9 | 37.2 | 43.7 | 44.1 | 20.0 | 17.8 |
| Median (mm) | 23.65 | 24.76 | 33.45 | 32.31 | 10.28 | 8.79 |
| Mean 士 SD (mm) | 23.6 士 5.4 | 24.6 士 5.5 | 34.2 士 4.4 | 33.3 士 5.5 | 10.6 士 4.2 | 9.3 士 4.3 |
| p-value* | 0.001 | 0.094 | 0.001 | |||
*Wilcoxon Signed Ranks.
The mean pre-extraction sagittal circumference of the sinus was 993.9 $\pm $ 295.7 mm, while post-extraction this sagittal circumference increased significantly to 1096.6 $ \pm $ 312.5 mm ($P<$ 0.0001).
When data were sorted by tooth type (Table 2), it was found that the mean pre-extraction floor-roof distances were 23.5 $ \pm $ 5.5 mm, 23.4 $ \pm $ 5.4 mm, and 24.0 $ \pm $ 5.9 mm for the first molar, second molar and second premolar sites, respectively. These differences were not statistically significant from the post-extraction distances of 23.8 $ \pm $ 5.5 mm, 24.9 $ \pm $ 5.4 mm, and 25.0 $ \pm $ 6.1 mm, respectively ($P=$ 0.95). Likewise, post-extraction BC-roof distance and BC-floor distance were not statistically different for the different extraction sites.
| Pre floor-roof | M1 | 23.5 | 士 | 5.5 | 10 | 0.95 |
|---|---|---|---|---|---|---|
| M2 | 23.3 | 士 | 5.4 | 14 | ||
| PM2 | 24.1 | 士 | 6.0 | 8 | ||
| Post floor-roof | M1 | 23.8 | 士 | 5.6 | 10 | 0.95 |
| M2 | 24.9 | 士 | 5.5 | 14 | ||
| PM2 | 25.0 | 士 | 6.2 | 8 | ||
| Pre BC-roof | M1 | 33.9 | 士 | 3.4 | 10 | 0.49 |
| M2 | 33.8 | 士 | 4.9 | 14 | ||
| PM2 | 35.4 士 | 5.0 | 8 | |||
| Post BC-roof | M1 | 32.6 | 士 | 4.9 | 10 | 0.49 |
| M2 | 32.4 士 | 6.0 | 14 | |||
| PM2 | 35.8 | 士 | 5.2 | 8 | ||
| Pre BC-floor | M1 | 10.6 | 士 | 4.3 | 10 | 0.48 |
| M2 | 9.8 | 士 3.5 | 14 | |||
| PM2 | 11.7 | 士 | 5.3 | 8 | ||
| Post BC-floor | M1 | 9.1 | 士 5.1 | 10 | 0.48 | |
| M2 | 8.4 士 3.7 | 14 | ||||
| PM2 | 11.1 | 士 | 4.4 | 8 | ||
M1, maxillary first molar; M2, maxillary second molar; PM2, Maxillary second premolar. *Wilcoxon Signed Ranks.
These data were further dichotomized by the nature of the procedure [i.e. extraction of single tooth versus extraction of multiple teeth (Table 3)]. Mean floor-roof dimension changes were slightly larger for the single extraction sites (range: 22.7 mm to 24.4 mm) compared to a range of 24.9 mm to 24.9 mm in the multiple extractions sites; however, both of these differences were not statistically significant ($P=$ 0.28 and 0.79, respectively). Similarly, no statistical difference was found in BC-roof (mean BC-roof dimension changes from 33.6 mm to 33.57 mm in single tooth and from 35.20 mm to 32.91 mm in multiple teeth extraction), and in BC-floor (mean BC-floor dimension changes from 10.7 mm to 9. 8 mm in single tooth, and from 10.3 mm to 8.6 mm in multiple teeth). Similarly, no difference was found in the sagittal circumference changes (996.4 $ \pm $ 308.0 mm pre-extraction to 1095.7 $ \pm $ 328.0 mm post-extraction, for single tooth extraction, and from 985.8 $ \pm $ 275.0 mm pre-extraction to 1099.6 $ \pm $ 277.0 mm post-extraction, for multiple teeth extraction, $P=$ 0.98).
| Single/multiple | Mean 士 SD (mm) | Teeth |
p-value* | |
|---|---|---|---|---|
| Pre floor-roof | Single | 22.7 士 5.6 | 20 | 0.28 |
| Multiple | 24.9 士 5.0 | 12 | ||
| Post floor-roof | Single | 24.4 士 6.1 | 20 | 0.79 |
| Multiple | 24.9 士 4.7 | 12 | ||
| Pre BC-roof | Single | 33.7 士 4.6 | 20 | 0.35 |
| Multiple | 35.2 士 4.1 | 12 | ||
| Post BC-roof | Single | 33.6 士 6.3 | 20 | 0.75 |
| Multiple | 32.9 士 3.9 | 12 | ||
| Pre BC-floor | Single | 10.7 士 4.1 | 20 | 0.78 |
| Multiple | 10.3 士 4.4 | 12 | ||
| Post BC-floor | Single | 9.8 士 4.2 | 20 | 0.45 |
| Multiple | 8.6 士 4.6 | 12 |
*Wilcoxon Signed Ranks.
The present study suggests that following the extraction of maxillary posterior teeth, sinus pneumatization occurs. Despite common conviction, there are only a few studies which investigated the phenomenon of maxillary sinus pneumatization in humans[4,5,17]. The measurement technique used in the present study helps minimizing possible inherent inaccuracies attributed to patient posture and the panoramic device itself. By superimposition of radiographic structures of known dimensions adjacent to the extraction area, it was possible to compare more accurately two different radiographs of the same subject taken at two different time points.
Mean sinus pneumatization in the vertical dimensions was found in the present study. The distance between pre and post sinus-floor to sinus-roof was increased in an average of 1 mm ($P=$ 0.001). In all these sites, pneumatization of the sinus was accompanied by an additional vertical resorption of an average 1.2 mm. Additionally, sinus sagittal circumference increased from a mean of 993.9 $ \pm $ 295.6 mm SD to a mean of 1096.6 $\pm $ 312.4 mm SD. These values of pneumatization are in agreement with a previous study showing an increase of 1.8 $ \pm $ 2.5 mm in sinus dimension for the same site pre- and post-extraction [5]. It should be noted that while we mostly found an increase in sinus height and circumference and a vertical resorption of the alveolar ridge, some studies reported opposite results.
The changes observed in the crestal bone height (BC-floor), are also in accordance with previous studies of the effect of tooth extraction on alveolar ridge height[13,16]. In these studies, tooth extractions led to a decrease in the alveolar bone height and width. It was observed that the bucco-lingual/palatal dimension during the first 3 months after tooth extraction was reduced by $\sim $30%, and after 12 months the edentulous site had lost at least 50% of its original width. Another systematic review found a mean crestal height change of $-$1.53 mm, 3-12 months post-extraction [18]. The vertical changes were predominantly of the buccal prominence, which has been shown to be located 1.2 mm apically to its lingual counterpart. The combination of these two phenomena may result in inadequate alveolar bone volume for further dental implants placement.
Both single and multiple extraction sites have shown an increase in the maxillary sinus and decrease in the crestal bone dimensions following tooth extraction, however with no statistically significant differences between the two groups. On the contrary, previous studies found a larger sinus expansion in cases in which multiple teeth were extracted in the same area in comparison to cases in which only one tooth was extracted and a larger decrease in alveolar ridge width, and more extensive bone remodeling after extracting two or more adjacent teeth, in comparison to a single tooth extraction[5,19]. This discrepancy might be due to different methodologies; while Sharan and Madjar used a personal computer screen framework in order to parallel the interorbital line prior to measurements [5], we superimposed and matched the two panoramic radiographs in order to compare the changes before and following tooth extraction. Al-Askar studied five female beagle dogs [19] while the current study was in humans.
The extraction of maxillary second pre-molar, first-molar and second-molar had similar effect on the linear change of the maxillary sinus and the crestal bone. Again, these findings do no concur with previous studies by Sharan and Madjar [5] and Wehrbein [4] who reported a larger expansion following extraction of Molar teeth compared to PM teeth. It should also be noted that Wehrbein quantified the progressive pneumatization of the basal maxillary sinus following extraction and orthodontic space closure [4].
The principal weakness of the present study is the use of panoramic radiographs to measure changes in alveolar ridge and maxillary sinus dimensions. Although reference points were used to accurately superimpose the two radiographs, the use of cone-beam computerized tomography (CBCT) could have reflected more accurately sinus pneumatization dimensions. Nevertheless, this study can be regarded as a starting point for the analysis of sinus pneumatization phenomenon which occurs following maxillary posterior teeth extraction. This phenomenon has been sparsely reported in the literature, and this study may shed light on changes following tooth extraction in the maxillary posterior region, which are associated with the maxillary sinus. Further studies including higher sample size and using CBCT should be conducted in order to validate these findings.
The results of the current study suggest that tooth extraction in the posterior maxilla is associated with an average 1.2 mm bone loss. These dimensional changes can be attributed to alveolar bone resorption as well as pneumatization of the maxillary sinus. These results are clinically relevant in the era of dental implants that require a minimum of 6 mm bone to stabilize the implant.
The present study was self-funded. No external funding was provided.
The authors whose names are listed above certify that they have no affiliations with, or involvement in, any organization or entity with any financial interest, or non-financial interest in the subject matter or materials discussed in this manuscript.