
Academic Editor: Márió Gajdács
Background and aims: Considering the advantages of rotary files in
instrumenting the root canals of permanent teeth and a lack of adequate data on
the use of these systems in primary teeth, the present study aimed to evaluate
two rotary files and compare them with hand files in the cleaning efficacy of
the root canals of primary molar teeth. Materials and methods: In the
present study, three groups of teeth were prepared with Kedo-S paediatric rotary
file system, RaCe (reamer with alternating cutting edges), and hand files (n =
40). The groups were evaluated under a stereomicroscope concerning the cleaning
efficacy of the files after cleaning the teeth in the apical, middle, and coronal
thirds. The data were analyzed with SPSS 24 (IBM Corporation, USA, 2016) using
Fisher’s exact test and chi-squared test; statistical significance was set at
p
A significant concern in pediatric dentistry is the premature loss of primary teeth despite efforts to prevent dental caries [1]. Premature loss of primary teeth is associated with complications such as space deficiency in the dental arch, masticatory and articulation disorders, esthetic problems, etc. Therefore, one of the most important aims in pediatric dentistry is to preserve posterior primary teeth until permanent teeth erupt [2, 3, 4]. The pulpectomy of primary teeth with pulpal inflammation is one of the therapeutic options to preserve space, function, and esthetic appearance [5].
Mechanical cleaning and shaping of the root canals of primary teeth are achieved through conventional and commonly used techniques with hand files. However, the manual preparation technique might lead to ledge formation, zipping, canal transportation, and other errors [2].
In 1999, the preparation of the root canals of primary teeth with rotary instruments was proposed by Barr for the first time [3]. Barr et al. [6] used Profile rotary files with 4% taper to instrument the root canals of primary teeth and showed that these files are useful and cost-effective for root canal preparation and lead to predictable and homogenous obturation of the root canal system.
The RaCe (reamer with alternating cutting edges) system consists of a complete set of rotary files for shaping and retreatment of the root canal system, which is easy to use. The special design of the files of this system prevents the screw-in effects and provides a better control of the instrument advancement for the endodontist, with proper flexibility and advancement in curved root canals. An innovation in the endodontic treatment in pediatric dentistry was the introduction of the Kedo-S paediatric rotary file system (Reeganz Dental Care Pvt. Ltd., India). It is a single-file system, consisting of D1, E1 and U1 files. The specific property of this file system is the different taper of the files (4–8%) and their different diameters considering their use in primary teeth.
Panchal et al. [7] compared the preparation time and obturation quality using K-files, H-files, and Kedo-S files in primary teeth in a randomized clinical trial and reported that Kedo-S files exhibited shorter preparation time and higher obturation quality compared to the two other file systems.
Ramazani et al. [8] carried out an in vitro study and reported the results of the evaluation of the cleaning efficacy, shaping ability, preparation time, and deformation of conventional files, the MTwo rotary system, and the single-file reciprocating Reciproc system in primary molars. Overall and in all the cases, rotary files exhibited better results than other files, with the reciprocating files preparing the root canals in the shortest time possible.
Different techniques, including cleaning after the injection of India ink and evaluating the amount of the smear layer removed, are used to evaluate the cleaning efficacy of different root canal preparation techniques. Cleaning after the injection of India ink is one of the most commonly used methods. In this method, India ink is injected before preparing the root canals. After root canal preparation and the cleaning process, the amount of the ink cleaned is evaluated under a stereomicroscope, which is an easy and inexpensive method for 3D observation of the tooth. This visual technique represents an alternative to the evaluation of the quality of the instrumentation performed with traditional imaging techniques such as CBCT or Micro CT or with advanced techniques, but which lately represent a rapidly evolving field such as MRI [9].
Considering the advantages of rotary files for instrumenting the root canals of permanent teeth and a lack of sufficient information about the results of the use of rotary systems in primary teeth, the present in vitro study was undertaken to evaluate and compare of the cleaning efficacy of Kedo-S and RaCe rotary file systems and the hand files in the root canals of primary molar teeth using the India ink technique.
In this in vitro study, the root canals of extracted primary second molar teeth were evaluated [10]. The sample size in each group was calculated at n = 40 based on previous studies by considering 0.5 value for first-level error and a study power of 90%. A total of 120 root canals of maxillary and mandibular primary second molar teeth were included in the study based on inclusion criteria and randomly assigned to three groups. There were equal members of corresponding root canals in the three study groups (Tables 1,2). Each group was given a number from 1 to 3. For randomization, an operator blinded to the study protocol and procedures assigned a number from 1 to 3 to the root canal preparation tools, based on which group allocation was carried out. For example, if the blinded operator assigned number 3 to the hand files, the teeth in group 3 were prepared with hand files.
| Group | Hand files | Kedo-S files | RaCe files | |||
| Tooth | No. | Percentage | No. | Percentage | No. | Percentage |
| Maxillary second molar | 15 | 46.8 | 18 | 48.6 | 20 | 55.5 |
| Mandibular second molar | 17 | 53.2 | 19 | 51.4 | 16 | 44.5 |
| Total | 32 | 100 | 37 | 100 | 36 | 100 |
| Group | Hand files | Kedo-S files | RaCe files | |||
| Molar | No. | Percentage | No. | Percentage | No. | Percentage |
| Maxillary mesiobuccal | 10 | 25 | 10 | 25 | 10 | 25 |
| Maxillary distobuccal | 10 | 25 | 10 | 25 | 10 | 25 |
| Mandibular mesiolingual | 10 | 25 | 10 | 25 | 10 | 25 |
| Mandibular mesiobuccal | 10 | 25 | 10 | 25 | 10 | 25 |
| Total | 40 | 100 | 40 | 100 | 40 | 100 |
(1) Primary second molar teeth with a minimum root length of 7 mm.
(2) Root canal curvature of
(3) No pathologic internal or external root resorption.
(4) No perforation of the furcal area.
Evaluation of resorption and the furcal area was carried out with an initial radiograph.
The selected teeth were rinsed under running water and then immersed in 0.5% chloramine T solution. After removing caries with a diamond fissure bur in a high-speed handpiece (Dentsply, Maillefer, Ballaigues, Switzerland), the access cavity was prepared, and the pulp chamber roof was removed. After irrigation of the pup chamber space with 1% NaOCl solution, a #10 K-file was placed in the root canal so that its tip was visible at the apical foramen. The working length (WL) was determined with a #15 K-file, one mm short of the root canal length. In the next stage, India ink was injected into the root canals using an insulin syringe so that it would exit from the root end. The teeth were mounted in acrylic resin so that the roots and tooth apices were not visible. Next, India ink was injected with an insulin syringe into the distal and palatal root canals as controls without root canal preparation and into the mesiobuccal and distobuccal root canals of maxillary molars and the mesiolingual and mesiobuccal root canals of mandibular molars as the test group (Fig. 1). Then, the samples were stored in humid conditions at room temperature for 48 hours [11].
 Fig. 1.
Fig. 1.Injection of India ink into the root canals with an insulin syringe.
Group 1: Root canal preparation was carried out manually with K-files (Dentsply, Maillefer, Ballaigues, Switzerland) (WL = 21 mm). In this group, root canal preparation was carried out with #15 to #30 files (D1) using the step-back technique.
Group 2: Root canal preparation was carried out with Kedo-S rotary files (Reeganz Dental Care, India), with the D1 file using the lateral brushing motion. An endomotor (NSK, ENDO-MATE, Japan) was used at 300 rpm at low torque (Fig. 2).
 Fig. 2.
Fig. 2.Kedo-S paediatric rotary files.
Group 3: Root canal preparation was carried out with RaCe rotary files (FKG Dentaire, Switzerland) with 2% taper with #15 to #30 files using the step-back technique. An endomoter (NSK, ENDO-MATE, Japan) was used at 300 rpm at low torque.
The root canals were irrigated with 1% NaOCl with a 27-G syringe (Endo Eze Ultradent Products Inc, South Jordan, UT), followed by irrigation with normal saline solution. A total of 10 mL of 1% NaOCl was used for each root canal [8]. The files were lubricated with 17% EDTA gel before inserting them into the root canals [10, 11, 12, 13]. The files were discarded and replaced with new ones after being used four times.
A pediatric dentistry postgraduate student who had been trained on the use of the rotary system carried out root canal preparation procedures under the supervision of an endodontist. Each session, only four root canals were prepared to prevent operator fatigue.
In the process of evaluating cleaning, after sealing the pulp chamber of the
samples with pink utility wax, the teeth were stored in a container containing
10% nitric acid for one day. The solution was renewed every 6 hours until the
teeth were decalcified. Then the teeth were rinsed under running water for 8
hours to completely remove the acid. Then the teeth were stored in 70% alcohol
for 16 hours for dehydration. The alcohol was renewed every 8 hours, followed by
immersion in 90% alcohol (which was renewed every hour) for 3 hours and in pure
alcohol (which was renewed every hour) for 3 hours. In the next stage, the teeth
were immersed in methyl salicylate (Merck, Germany) to achieve a transparent
appearance [13]. After the cleaning process, the amount of removed India ink was
evaluated in the coronal, middle, and apical thirds under a stereomicroscope at
0: Complete removal of the ink from all the root canal walls.
1: Some ink has been removed.
2: No ink has been removed.
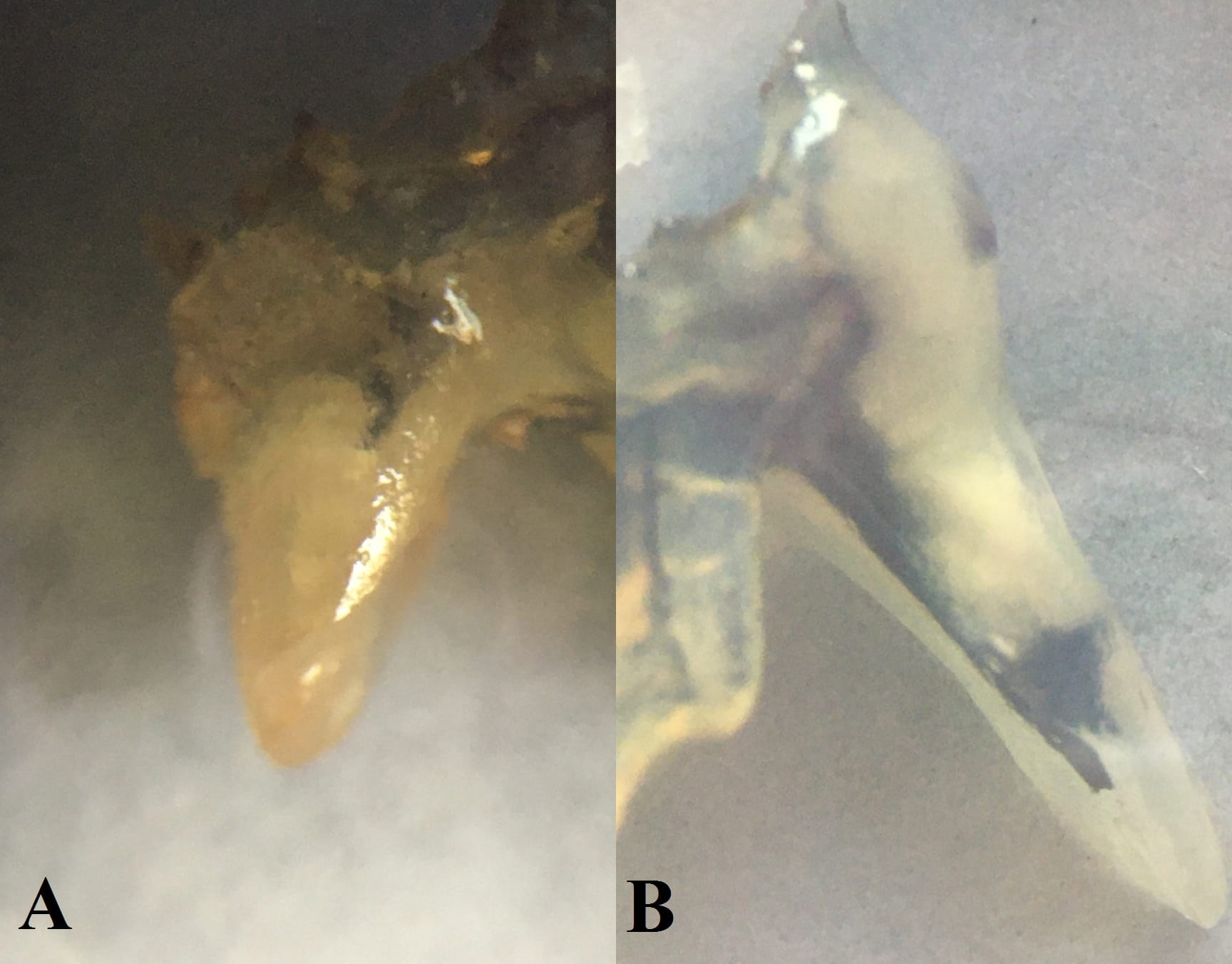 Fig. 3.
Fig. 3.A stereomicroscopic image of a sample. (A) The coronal, middle, and apical area, grade 0. (B) The coronal and middle area, grade 2; the apical area, grade 0.
Blindly, two trained dentists scored the group allocation in the each sample at the coronal, middle, and apical portion of each canal [14].
The data were analyzed with SPSS 24 (IBM Corporation, USA, 2016) using Fisher’s
exact test and chi-squared test. Statistical significance was set at p
The samples evaluated in the present study consisted of 120 root canals in
extracted primary maxillary and mandibular second molar teeth. The root canals
were prepared in three groups using Kedo-S and RaCe rotary files and manual
K-files. The results were reported as follows (Tables 3,4,5,6). Interobserver
agreement was 0.827 (p
Fisher’s exact test and the p-values indicated no significant differences in the cleaning efficacy in the apical area between the different study groups (Table 3).
| Group | Hand files | Kedo-S files | RaCe files | |||
| Cleaning efficacy | No. | Percentage | No. | Percentage | No. | Percentage |
| 0 | 28 | 70 | 34 | 83.7 | 28 | 70 |
| 1 | 10 | 25 | 6 | 16.3 | 9 | 22.5 |
| 2 | 2 | 5 | 0 | 0 | 3 | 7.5 |
| p = 0.336 | ||||||
Fisher’s exact test and the p-values indicated significant differences in the cleaning efficacy in the middle third between the different study groups (Table 4).
| Group | Hand files | Kedo-S files | RaCe files | |||
| Cleaning efficacy | No. | Percentage | No. | Percentage | No. | Percentage |
| 0 | 21 | 53.8 | 30 | 75 | 27 | 67.5 |
| 1 | 14 | 33.3 | 10 | 25 | 10 | 25 |
| 2 | 5 | 12.8 | 0 | 0 | 3 | 7.5 |
| p = 0.099 | ||||||
Chi-squared test and p-values indicated significant differences in cleaning efficacy in the coronal area between the different study groups (Table 5).
| Group | Hand files | Kedo-S files | RaCe files | |||
| Cleaning efficacy | No. | Percentage | No. | Percentage | No. | Percentage |
| 0 | 21 | 52.5 | 28 | 70 | 25 | 62.8 |
| 1 | 12 | 30 | 2 | 5 | 12 | 32.6 |
| 2 | 7 | 17.5 | 10 | 25 | 3 | 4.7 |
| p = 0.005 | ||||||
Fisher’s exact test showed no significant differences between the hand files and the RaCe rotary files in the cleaning efficacy in the coronal area in different groups. However, chi-squared test showed significant differences between the Kedo-S and RaCe files and the Kedo-S and hand files (Table 6).
| Comparison | p-value |
| RaCe files vs. hand files | 0.181 |
| Kedo-S files vs. RaCe files | 0.001 |
| Kedo-S files vs. hand files | 0.016 |
There is a professional tendency among pediatric dentists to facilitate pulp treatments more efficiently. Thus biomechanical primary teeth root preparation with a rotary system was first introduced by Barr et al. [6] in 2000. There is no standard protocol regarding primary root canal preparation using rotary systems and application of this protocol in primary teeth may cause unintentional perforations [8]. In the present study, root canals of primary second molar with fewer anatomical variations were used. These included mesiobuccal and distobuccal root canals of maxillary and mesiobuccal and mesiolingual root canals of mandibular primary second molar teeth. Due to the greater importance of primary second molar teeth in the development of occlusion in comparison with first primary molars, second molar teeth were used in the present study. Other canals of these teeth were used as the control groups to ensure dye penetration, similar to study by Madam et al., and previously evaluated in the literature [13, 15, 16]. Study groups matched regarding canal type as possible. Teeth with a minimum root length of 7 mm were included in the study to evaluate the cleaning and shaping efficacy of the root canal preparation tools, consistent with a study by Silva et al. [17].
Since variations in canal curvature might affect the study results, the samples were limited to teeth with 10–20º curvature. In addition, the groups were assigned to the study groups randomly.
Since the main goal of root canal treatment in primary teeth is cleaning rather than shaping [6], and the present study is designated to evaluate the cleaning efficacy of different systems, the India ink clearance technique used the same as some previous studies [13].
Studies have suggested rotary files with a maximum taper of 4% to prepare the root canals of primary teeth because greater taper results in a higher torque and file fracture [18, 19]. Musale et al. [10] suggested that root canal preparation with instruments having 4–6% taper and an apical diameter of 0.2–0.3 mm are approximate for primary molars. In the present study, Kedo-S files with a varying taper of 4–8% and RaCe files with 2% taper were used.
Some studies have suggested the crown-down technique for root canal preparation. However, Barr et al. [6] believe that this technique is not necessary for the preparation of primary teeth because the dentin in primary teeth can be cut easier than that in permanent teeth, which was confirmed by Silva et al. [17], who used the step-back technique to prepare primary teeth.
Preflaring with Gates-Glidden drills has been suggested before preparing the root canals in permanent teeth with the step-back technique; however, this technique is not suggested in primary teeth because it increases the risk of perforation [20].
The results of the present study showed no significant differences in the cleaning efficacy in the apical and middle thirds between the different study groups.
The Kedo-S file system was significantly more effective than hand files (p = 0.016) and RaCe files (p = 0.001) except for the coronal third. However, such a difference between the hand files and RaCe files was not significant.
In the present study, the Kedo-S file system was significantly more effective than the hand and RaCe files in cleaning the coronal third; however, in the apical and middle thirds, the results of the present study were similar to those in most previous studies.
In the study by Madam et al. [13], the Profile system was more effective in the coronal third, and the K-file system was more effective in the apical third. However, in the middle third, the two systems exhibited similar efficacy, consistent with the present study in the coronal and middle thirds. However, the results of the above study in the apical third were contrary to most previous studies, which might be attributed to differences in the file systems used and the teeth evaluated [9].
The results of the present study showed no significant difference in the cleaning efficacy in the apical and middle areas between the different study groups, this is an important guarantee of effective endodontic obturation [21]. However, the Kedo-S system was significantly more effective than the hand and RaCe files.
In primary teeth, due to the abundance of the accessory root canals in the coronal area (reflects in more common radiolucencies in furcal area rather than apical area) and physiologic resorption of the apical area, cleaning the apical area is not challenging; instead, cleaning the coronal and middle thirds is more important [8, 11]. Due to an increase in the diameter of dentinal tubules and the softness of the dentin in the coronal area, if rotary files are used, the dentin is removed more easily compared to the hand files, which might be an important factor in increasing the cleaning efficacy of rotary files in the coronal area than the apical and middle areas [8, 13]. On the other hand, this finding can be explained by the other characteristics of the root canal. Although the root canals of primary molars are wide buccolingually, it can be inferred that in the coronal area, there is a higher adaptation and harmony between the root canal cross-section and rotary files [8, 11, 17]. The higher efficacy of rotary files in cleaning the coronal area can be an essential advantage of rotary files in preparing the root canals in primary molars because, as explained above, in the coronal areas, the cleaning efficacy of the tools is very important due to the presence of accessory root canals. In the present study, Kedo-S files were more effective than the hand and RaCe files, which might be an essential advantage for Kedo-S files.
Although using human extracted teeth can somehow examine the performance of different instruments, the in vitro nature of the present study was a limitation due to significant differences from the clinical condition, which should be considered in future studies.
The present study showed that Kedo-S files were more effective than the hand and RaCe files in cleaning the coronal area. However, there were no significant differences in the cleaning efficacy in the apical and middle thirds between the different study groups. Considering the in vitro nature of the present study and the differences in conditions, including limitations in children’s compliance and mouth opening degree, it is not logical to extend the findings to clinical conditions.
Conceptualization—MT, AE, MA, RR; methodology—MT, AE, MA, FK, LT; validation—MT, AE, MA, FK, LT; formal analysis—NM; investigation—MT, AE, FK; resources—MA, FK; data curation—FK, AE; writing—original draft preparation—MT, RR, LT; writing—review and editing—LT; visualization—MT; supervision—MT, AE, LT; All authors have read and agreed to the published version of the manuscript.
The study protocol was approved by the Ethics Committee of Qazvin University of Medical Sciences under the code IR.QUMS.REC.1398.73.
The authors would like to thank Razieh Jabbarian and Tina Bakhtiari for their valuable contribution in this study.
This research received no external funding.
The authors declare no conflict of interest. LT is serving as one of the Editorial Board members of this journal. We declare that LT had no involvement in the peer review of this article and has no access to information regarding its peer review. Full responsibility for the editorial process for this article was delegated to MG.