

 , Fengzhen Li 2, Ping Lu 2, Yushuang Yao 1, Huaqin Sun 1, Zhaoxia Ding 1,*
, Fengzhen Li 2, Ping Lu 2, Yushuang Yao 1, Huaqin Sun 1, Zhaoxia Ding 1,*
1 Department of Gynecology, The Affiliated Hospital of Qingdao University, 266000 Qingdao, Shandong, China
2 Department of Gynecology, Zhucheng People’s Hospital, 262200 Zhucheng, Shandong, China
Abstract
The factors associated with high-risk human papillomavirus (HR-HPV) clearance and its regulation following conization of cervical HPV-associated lesions remain unclear.
Information was extracted on patients who underwent cold knife conization (CKC) or loop electrosurgical excision procedure (LEEP) at the Affiliated Hospital of Qingdao University and Zhucheng People’s Hospital between September 2014 and September 2020. We compared postoperative HR-HPV clearance between the CKC and LEEP groups using Kaplan-Meier (K-M) curves and calculated the restricted mean survival time (RMST) for each group. Subsequently, we employed univariate and multivariate logistic regression analyses to determine independent prognostic factors.
In total, 339 patients were enrolled, including 182 patients who underwent CKC (53.7%) and 157 patients who underwent LEEP (46.3%). The HPV16/18 regression rates were 92.2% and 85.7% in the CKC and LEEP groups, respectively. Patients who underwent LEEP experienced a longer HR-HPV regression period than those who underwent CKC, along with significantly lower regression rates [hazard ratio (HR): 0.795; 95% confidence interval (CI): 0.223–0.974; p = 0.049]. The RMST of HR-HPV positivity after surgery was 5.23 months in the CKC group and 5.79 months in the LEEP group (p = 0.463). Multivariable analysis identified LEEP as an independent risk factor for persistent positive HR-HPV after surgery (odds ratio (OR): 5.730; 95% CI: 1.236–26.568; p = 0.026).
CKC is associated with faster, more complete clearance of HR-HPV compared with LEEP. Procedure selection should prioritize adequate excision while preserving healthy tissue. Nonetheless, prospective, standardized studies are needed to confirm these findings.
Keywords
- high-risk human papillomavirus
- squamous intraepithelial lesion
- cold knife conization
- loop electrosurgical excision procedure
- virus regression
Cervical cancer is a malignancy that poses a significant risk to the health of women. It ranks fourth worldwide in terms of both incidence and mortality, with a higher incidence in developing countries than in developed countries [1]. Persistent cervical infection with high-risk human papillomavirus (HR-HPV) leads to the development of precancerous lesions known as high-grade squamous intraepithelial lesions (HSIL) and adenocarcinoma in situ (AIS), which may ultimately lead to cervical cancer [2].
Individuals diagnosed with early-stage cervical carcinoma and precancerous lesions often undergo conization treatment, predominantly cold knife conization (CKC) and the loop electrosurgical excision procedure (LEEP) [3]. A small number of patients with persistent HR-HPV infection or low-grade squamous intraepithelial lesions (LSIL) require diagnostic conization. For patients with HPV-associated lesions who undergo cervical conization, regular postoperative monitoring of HR-HPV infection and cytology is essential for early detection of persistent HR-HPV infection and diagnosis of residual or recurrent disease [4, 5, 6]. Persistent HPV infection plays a critical role in the recurrence risk following CKC and LEEP. Studies indicate that postoperative HPV persistence is closely associated with the recurrence risk of cervical intraepithelial neoplasia (CIN), particularly with persistent infection by HPV16 being recognized as a significant predictor of CIN2+ recurrence [7, 8]. In postoperative follow-up studies of LEEP procedures, early HPV testing has been proven to be an effective predictor of residual or recurrent lesions. Research indicates that HPV testing conducted 3 months after surgery can accurately identify all residual or recurrent cases, achieving 100% sensitivity and negative predictive value [9]. Furthermore, the relationship between persistent postoperative HPV infection and surgical margins has been extensively investigated. Even when surgical margins were negative, persistent HPV infection significantly increased the risk of CIN recurrence [10]. A meta-analysis revealed that 22.7% of patients had residual HPV after surgery, with CIN recurrence rates remaining substantially elevated even in cases of negative margins [10]. These findings underscore the critical importance of addressing persistent postoperative HPV infections.
Post-conization surveillance relies on HR-HPV and cytology to detect residual or recurrent disease. However, whether the excisional modality itself influences genotype-specific HR-HPV clearance or persistence remains uncertain. As CKC and LEEP differ in thermal artifact, specimen integrity, and typical cone dimensions, they may differentially affect viral reservoirs and, consequently, clearance dynamics. To date, only a few studies have compared the effects of CKC and LEEP on HR-HPV regression and the influencing factors in patients after conization [11]. Therefore, we aimed to investigate the factors associated with clearance of HR-HPV in patients with cervical HPV-associated lesions following conization and to provide insights that can guide the implementation of more targeted treatment action plans in the future.
A retrospective review was conducted on 339 patients with cervical lesions treated with either CKC or LEEP at the gynecology departments of the Affiliated Hospital of Qingdao University and Zhucheng People’s Hospital between September 2014 and September 2020.
Inclusion criteria: (1) Histopathologically confirmed cervical precancerous lesions before treatment, including CIN and AIS, as reported by the local pathology service. (2) Treated with CKC or LEEP as the sole excisional therapy for the index lesion during the study period at one of the two participating hospitals. (3) Post-procedure follow-up performed per institutional protocol with HR-HPV genotyping and ThinPrep cytology test (TCT) at the prespecified intervals.
Exclusion criteria: (1) Any primary treatment other than CKC or LEEP alone for the index lesion, or CKC/LEEP performed concomitantly with other definitive cervical procedures. (2) Loss to follow-up. (3) Prolonged immunosuppression or known primary or secondary immune disorders that are likely to affect HPV clearance or cytology results.
All surgeries were performed following standard clinical protocols for CKC and LEEP. The treatment area for both procedures was clearly defined, with surgical margins carefully marked to ensure complete resection of the cervical lesion. The size and location of the treatment area were tailored to the lesion to guarantee adequate coverage for complete removal. All procedures adhered to the National Comprehensive Cancer Network (NCCN) guidelines, which are widely accepted for these treatments. The surgeries were performed by a team of experienced gynecologists at the Affiliated Hospital of Qingdao University and Zhucheng People’s Hospital. All surgeons had extensive experience with CKC and LEEP procedures, each with a minimum of 10 years of practice. Additionally, training and skill levels were comparable across both institutions, ensuring consistency in surgical techniques and patient management throughout the study period. The participating surgeons were all members of established gynecological departments and regularly performed conization procedures during the study.
After a rigorous screening process based on the inclusion criteria, 339 patients were selected, including 157 LEEP cases and 182 CKC cases (Fig. 1).
 Fig. 1.
Fig. 1.
The flow chart of this study. CKC, cold knife conization; LEEP, loop electrosurgical excision procedure.
These individuals were monitored at regular intervals for 4–6 months after the procedure. Cervical HR-HPV typing and TCT were performed regularly at follow-up. When both HR-HPV and TCT were negative, the follow-up interval was extended to 1 year. This retrospective, longitudinal follow-up study recorded the symptoms and positive signs of all patients. By reviewing the inpatient and outpatient medical records and related laboratory and examination results, information on demographic data, disease history, treatment of cervical lesions, preoperative HR-HPV and TCT results, postoperative HR-HPV and TCT results, and patient age were collected. An SPSS 20.0 (IBM Corp., Armonk, NY, USA) patient information database was also established.
An automated liquid-based cytology (LBC) technology, SurePath™ liquid-based Pap test (Becton Dickinson, Franklin Lakes, NJ, USA), was employed for the cytological examination, while immuno-cytochemistry utilized tris-buffered saline. All samples were interpreted by an experienced cytopathologist using the 2001 Bethesda System.
The identification and classification of HPV was conducted using a commercially available Yaneng Organisms system (YanengBIO, Shenzhen, Guangdong, China), employing a polymerase chain reaction method capable of detecting 35 different HPV genotypes. This method is capable of concurrently identifying both high-risk HPV types (16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82) and low-risk HPV types (6, 11, 40, 42, 43, 44, 54, 61, 62, 70, 71, 72, 81, 83, 84, 85, and 89).
All colposcopy images were obtained using high-definition electronic colposcopes, and colposcopy and colposcopy-guided biopsy were performed by two expert colposcopists with more than 10 years of clinical experience, according to the standard protocol. The fixed specimens were sent to the pathology department for examination.
The pathological sections were examined by two pathologists with gynecological pathology experience, and when there were disagreements in the results, the sections were reviewed by more experienced doctors. The lesion degree was based on the highest pathological grade.
(1) Persistent infection: Presence of the same HR-HPV genotype on
(2) Transient infection: Any HR-HPV genotype-positive episode that does not meet
the definition of persistence (i.e., duration
(3) Virus regression: For a previously positive genotype, two consecutive
negative tests
(4) Virus regression time: Persistent virus infection followed up again to determine the time of virus regression or type change, with the first negative time as the time node.
(5) Recurrent infection: After clearance of any genotype, new detection of HR-HPV (same or different genotype).
(6) Time of recurrent infection: The interval from the clearance date to the date of the first subsequent positive test.
Statistical analyses were performed using SPSS 20.0. Normally
distributed continuous data were represented as means
As shown in Table 1, of the 339 patients, 103 undergoing CKC tested positive for HPV16/18 before the procedure. Patients in both the conization and LEEP groups were monitored consistently over a period ranging from 1 to 96 months, with a median follow-up duration of 12 months. Of the 339 patients, 307 had evaluable postoperative follow-up data, and 243 were persistently negative, accounting for 79.2% of the total. 31 patients presented with transient infection (10.1%) and 24 presented with persistent infection (7.8%). As shown in Tables 1,2, the postoperative clearance rates of HPV 16/18 were 92.2% in the CKC group and 85.7% in the LEEP group. For other HR-HPV types, the postoperative clearance rates were 91.8% in the CKC group and 82.5% in the LEEP group. These differences were statistically significant (p = 0.004). For cases with missing data, we conducted a statistical analysis comparing their baseline characteristics to those of cases with complete data and found no significant differences.
| Characteristics | CKC (n = 182) | LEEP (n = 157) | p-value | |
| Age (years) | 40.0 |
37.3 |
0.004 | |
| Menopause | 0.228 | |||
| Yes | 161 | 145 | ||
| No | 21 | 12 | ||
| Preoperative HPV genotype | 0.618 | |||
| 16/18 | 103 | 91 | ||
| Other HR-HPV types | 61 | 57 | ||
| Low-risk HPV types | 8 | 4 | ||
| Negative | 1 | 1 | ||
| Missing | 9 | 4 | ||
| Preoperative TCT grade | 0.399 | |||
| 68 | 59 | |||
| 59 | 28 | |||
| Missing | 55 | 70 | ||
| Pathological grade | ||||
| 4 | 45 | |||
| HSIL | 133 | 102 | ||
| AIS | 35 | 10 | ||
| Infiltrating carcinoma | 10 | 0 | ||
AIS, adenocarcinoma in situ; HPV, human papillomavirus; HSIL, high-grade squamous intraepithelial lesions; LSIL, low-grade squamous intraepithelial lesions; HR-HPV, high-risk human papillomavirus; TCT, ThinPrep cytology test.
| Characteristics | CKC (n = 182) | LEEP (n = 157) | p-value | |
| Median follow-up time (months) | 12 | 12 | 0.214 | |
| Postoperative HPV regression | 0.004 | |||
| 16/18 | 95 (59.0%) | 78 (53.4%) | ||
| Other HR-HPV types | 56 (34.8%) | 47 (32.2%) | ||
| Low-risk HPV types | 6 (3.7%) | 1 (0.7%) | ||
| No | 4 (2.5%) | 20 (13.7%) | ||
| Missing | 21 | 11 | ||
| Postoperative HR-HPV | 0.023 | |||
| Persistent negative | 130 (79.8%) | 113 (77.4%) | ||
| Persistent infection | 4 (2.5%) | 20 (13.7%) | ||
| Recurrent infection | 8 (4.9%) | 3 (2.0%) | ||
| Transient infection | 21 (12.9%) | 10 (6.8%) | ||
| Missing | 19 | 11 | ||
| Postoperative HR-HPV regression time | 0.049 | |||
| 1–3 months | 82 (52.9%) | 75 (54.7%) | ||
| 4–6 months | 48 (31.0%) | 33 (24.1%) | ||
| 7–12 months | 21 (13.5%) | 25 (18.2%) | ||
| 13–24 months | 4 (2.6%) | 4 (2.9%) | ||
The median time to viral extinction in the CKC and LEEP groups was 5.4 months and 5.9 months, respectively. Log-rank survival analysis showed that the postoperative regression times of the two groups were different, and the postoperative viral regression of patients in the LEEP group was slower than that in patients in the CKC group (Fig. 2). However, the difference in the postoperative cumulative positive rate of HR-HPV between these two groups was not significant (Fig. 3). Additionally, the RMST of HR-HPV positivity after surgery in the CKC and LEEP groups was 5.23 and 5.79 months, respectively, with a p-value of 0.463 (Fig. 4).
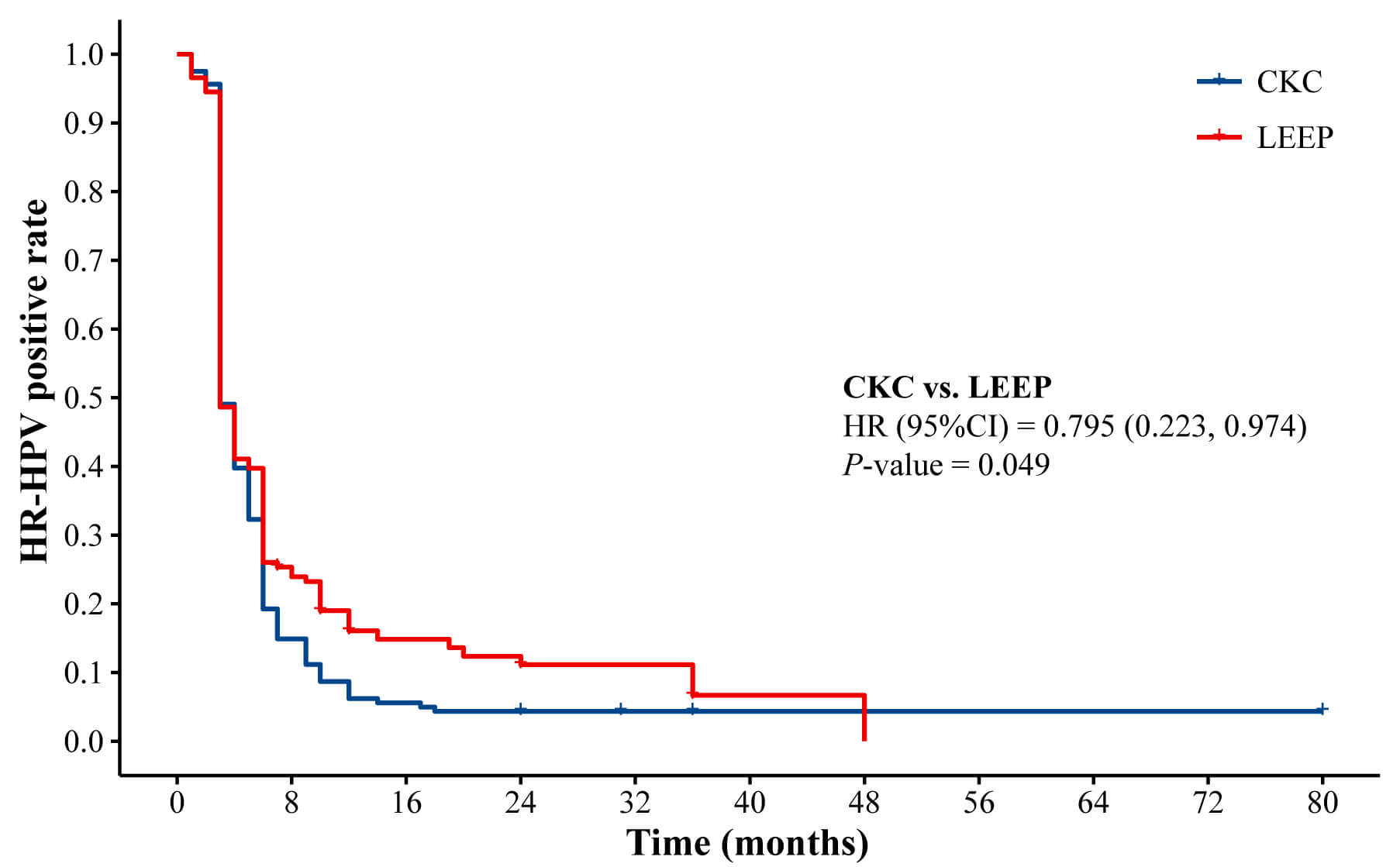 Fig. 2.
Fig. 2.
Postoperative viral infection rate in patients of CKC and LEEP. CI, confidence interval; HR, hazard ratio.
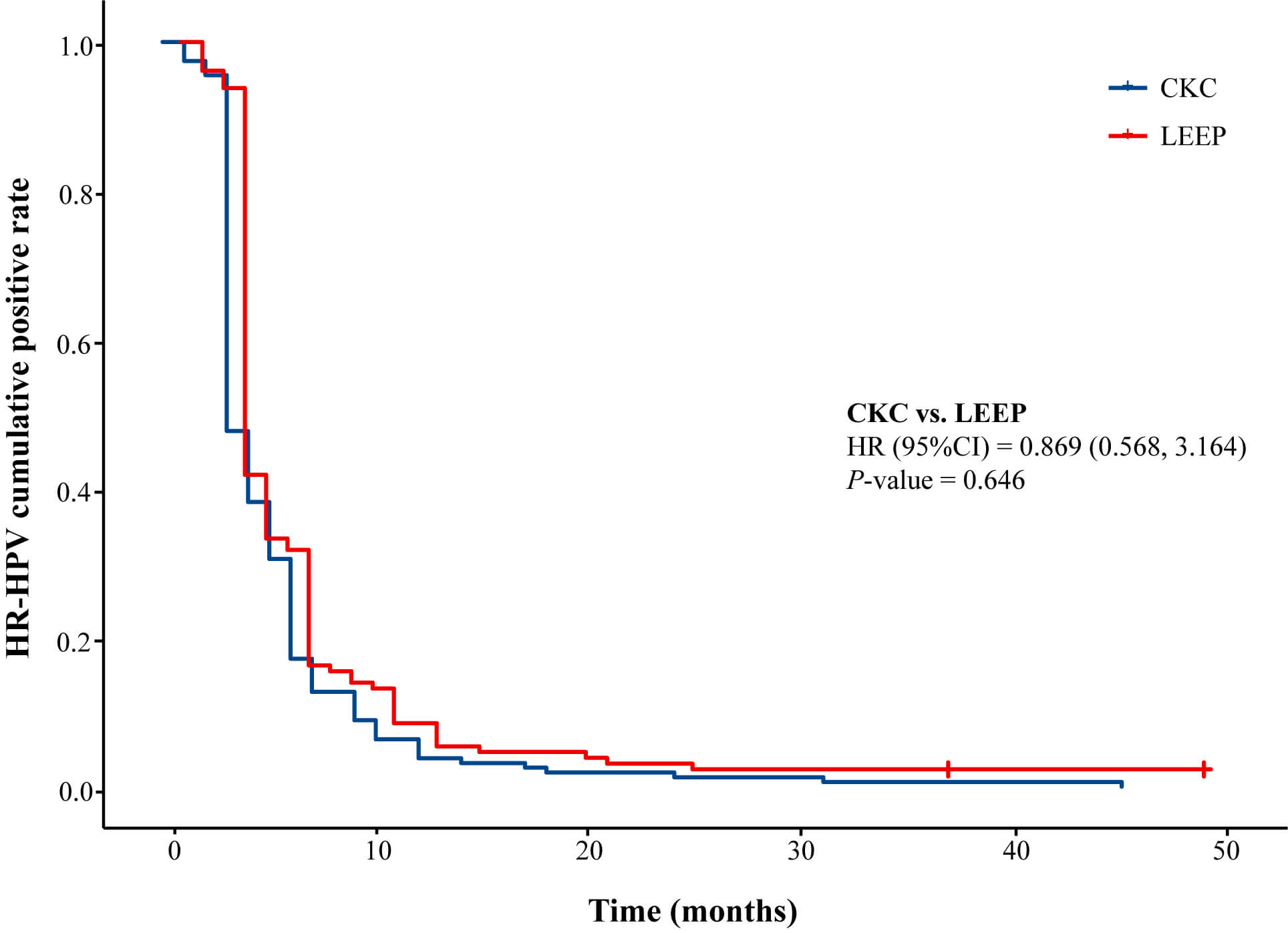 Fig. 3.
Fig. 3.
Postoperative cumulative viral infection rate in patients of CKC and LEEP.
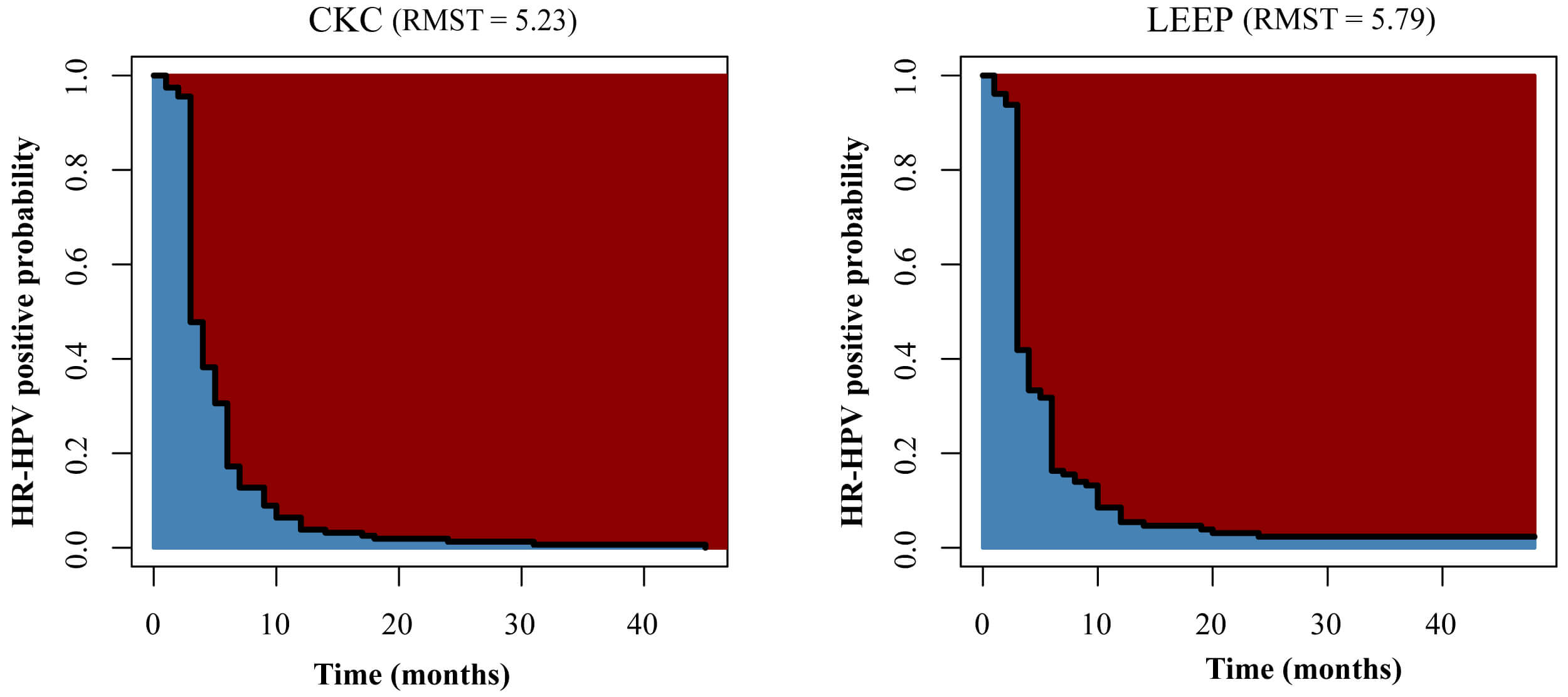 Fig. 4.
Fig. 4.
RMST of postoperative viral infection rate in patients of CKC and LEEP. RMST, restricted mean survival time.
Univariate analysis showed that the preoperative TCT grade (p = 0.021) and surgical procedure (p = 0.001) were related to the presence or absence of the virus (Table 3). And we did not find an association between HPV genotypes and the surgical method (chi-square value = 12.306, p = 0.677). Subsequently, we included the preoperative TCT grade as a covariate to account for its potential confounding effect on the association between the surgical procedure and persistent HPV infection. Multivariate logistic regression analysis of risk factors associated with persistent HR-HPV infection indicated that LEEP was an independent risk factor for persistent positive HR-HPV status postoperatively (p = 0.026) (Table 4).
| Factors | Non-persistent positive (n = 283) | Persistent positive (n = 24) | p-value | |
| Age (years) | 38.7 |
36.8 |
0.318 | |
| Menopause | 1.000 | |||
| No | 255 (90.1%) | 22 (91.7%) | ||
| Yes | 28 (9.9%) | 2 (8.3%) | ||
| Operation | 0.001 | |||
| CKC | 157 (55.5%) | 4 (16.7%) | ||
| LEEP | 126 (45.5%) | 20 (83.3%) | ||
| Margin | 0.598 | |||
| Negative | 273 (96.5%) | 23 (95.8%) | ||
| Positive | 10 (3.5%) | 1 (4.2%) | ||
| Postoperative multiple HR-HPV infection | 0.058 | |||
| Yes | 54 (58.7%) | 4 (30.8%) | ||
| No | 38 (41.3%) | 9 (69.2%) | ||
| Missing | 191 | 11 | ||
| Postoperative HPV types | 0.761 | |||
| 16/18 | 63 (66.3%) | 8 (61.5%) | ||
| Others | 32 (33.7%) | 5 (38.5%) | ||
| Missing | 188 | 11 | ||
| Preoperative TCT grade | 0.021 | |||
| 101 (61.6%) | 16 (88.9%) | |||
| 63 (38.4%) | 2 (11.1%) | |||
| Missing | 119 | 6 | ||
| Pathological grade | 0.227 | |||
| 40 (14.1%) | 6 (25.0%) | |||
| 243 (85.9%) | 18 (75.0%) | |||
| Factors | Wals | OR | 95% CI for OR | p-value |
| Preoperative TCT ( |
2.009 | 0.326 | 0.069–1.536 | 0.156 |
| Surgery (CKC vs. LEEP) | 4.976 | 5.730 | 1.236–26.568 | 0.026 |
OR, odds ratio.
Cervical cancer is the most prevalent malignant tumor. Since the 1990s, a research study has demonstrated a strong association between HR-HPV infections and cervical cancer [12]. Nonetheless, HR-HPV infections in the epithelial cells of the female reproductive system are quite prevalent, with the majority being temporary, symptomless, and typically eliminated by the immune system within 6–24 months. Only a small number of persistent cases result in cervical abnormalities [13]. Disease progression occurs in a specific sequence, starting with an initial HPV infection and moving through various stages of cervical lesion formation, before culminating in cervical cancer. This progression takes approximately 8–12 years [14]. The molecular mechanisms underlying HPV treatment and persistent infection remain an active area of research. A recent study has indicated that post-translational modifications (PTMs), such as lysine succinylation, play a significant role in regulating antiviral immunity, which may help explain the persistence of HR-HPV infections [15]. Timely intervention during the precancerous phase is crucial for lowering the incidence and death rates associated with cervical cancer. In 2015, Joste and colleagues [16] observed a notable reduction in HPV infection rates within 3 months post-surgery among patients with HSIL who underwent CKC. In this study, the postoperative disappearance rates of HPV16/18 were 92.2% in the CKC group and 85.7% in the LEEP group. This decline could be attributed to lesion removal, enhanced local immune response, and improved self-clearance of the virus, leading to a significant decrease in HPV levels in the reproductive tract. Notably, our HPV clearance rate is higher than that reported in previous studies. For example, a retrospective study demonstrated that 64.5% of patients undergoing conization achieved complete HPV clearance [17]. Additionally, another study reported HPV clearance rates of 24.5% at 6 months and 67.9% at 12 months post-treatment [18]. This may be attributable to regional differences and variations in healthcare resources. Furthermore, the findings of this study indicate a notable statistical disparity in the regression duration of HR-HPV between the CKC and LEEP procedures, with patients undergoing LEEP experiencing a longer regression period than patients undergoing CKC, suggesting potential differences in the therapeutic outcomes of CKC and LEEP for patients with cervical lesions. A possible reason for this is that CKC has a wider scope for cervical resection, and the resection effect is more reliable. At the same time, we observed similar postoperative cumulative positive rates of HR-HPV and RMST between the two groups, with no statistically significant differences. This may be due to censoring and follow-up biases.
Earlier research has indicated that numerous factors, such as age, single or multiple infections, and infection genotyping, are associated with HPV infection and its resolution [19, 20]. A study conducted in Western Kazakhstan reported a prevalence of HR-HPV types at 26%, which was lower than the prevalence found in our study [21]. This difference may be attributed to variations in the popularity and standardization of cervical cancer screening programs. Nevertheless, our findings are consistent with this study, as both indicate a relatively high prevalence of HR-HPV types among women with cervical lesions [21]. Notably, several markers have been identified as indicators of poor prognosis in HPV-related diseases, including squamous cell carcinoma antigen (SCC Ag), which has been shown to predict unfavorable treatment outcomes in patients with cervical cancer [22]. In recent years, with the progress of the research in the field of HR-HPV, the significance of postoperative outcomes in terms of the progression of cervical lesions has become increasingly clear. Some studies have shown that HR-HPV infection is a risk factor for residual lesions and recurrence after conization. This may be because, in patients whose cervical lesions have been removed but the virus persists, HR-HPV can remain hidden and re-infect the stump epithelium, resulting in persistent HR-HPV infection after surgery [4, 5, 20, 23]. An observational study indicated that patients with HPV 16 infection and a high viral DNA load experience slower viral clearance [24], while another study identified age as a prognostic factor for the clearance of HR-HPV infections after surgery [25]. In addition, a study by Venturoli et al. [26] evaluated several clinical and viral factors, including HPV16 infection and a positive cutting edge, but found no factors affecting virus clearance time. Therefore, no conclusion exists on the negative conversion time of HR-HPV, the various types of HR-HPV, and the high-risk factors affecting negative conversion. In our study, we found that patients in the CKC group had a lower risk of postoperative persistent HR-HPV infection than those in the LEEP group. This finding is consistent with a previous study that reported a higher positive rate of postoperative cervical secretion HPV infection in the LEEP group compared to the CKC group. However, Chen et al. [27] and Jiang et al. [28] found there was no difference in these two groups. Galli et al. [29] also found that women undergoing the LEEP procedure showed no statistically significant difference compared to those undergoing CKC in terms of persistent disease and positive margins. Additionally, they had a lower risk of postoperative bleeding within 24 hours [29]. Higher HPV clearance after CKC may reflect a deeper, en bloc excision with clearer margin assessment, which enhances the removal of endocervical crypt reservoirs. In contrast, thermal artifacts and piecemeal excision associated with LEEP can hinder complete clearance. However, when LEEP achieves adequate depth with negative margins, the differences between the two procedures become minimal [30, 31]. These results indicate that, whether CKC or LEEP is performed, oncologic adequacy must be balanced with the preservation of normal tissue to ensure sufficient excision with minimal collateral damage. Recent advancements in intelligent nanomaterials have opened new avenues for targeted therapies, particularly for HPV-related diseases [32]. These nanomaterials can be engineered to specifically target HPV-infected tissues, thereby enhancing therapeutic efficacy while minimizing off-target effects.
This study had several limitations. First, the retrospective, single-center design is susceptible to confounding by indication and unmeasured variables. The clinical decision to perform CKC versus LEEP may be influenced by factors that also affect HPV clearance. Although available covariates were accounted for, residual confounding is likely. Second, selection bias may be present. Excluding patients who did not undergo CKC or LEEP, or those lost to follow-up, could result in a sample enriched with more adherent patients who have better outcomes; this informative censoring could bias clearance estimates. Third, the follow-up duration was relatively short and variable, which may lead to underestimation of late clearance or recurrence and potential misclassification of persistence when testing intervals are prolonged.
In this retrospective cohort study of women treated with cervical conization, CKC resulted in higher genotype-specific clearance of HR-HPV and a shorter time to regression compared to the LEEP. Multivariable analysis revealed that LEEP was independently associated with persistent postoperative HR-HPV positivity, whereas factors such as age, menopausal status, mixed infections, and margin status were not. These findings underscore the importance of achieving oncologically adequate excision by ensuring sufficient cone depth and volume with clear margins, while minimizing damage to uninvolved tissue, regardless of the procedure used. Future prospective studies should focus on determining the factors influencing postoperative HPV clearance to provide even stronger evidence to guide clinical decision-making.
The datasets generated during and analysed during the current study are available from the corresponding author on reasonable request.
YS: Data analysis, drawing figures and tables, writing original draft. FL: Data analysis. PL: Drawing figures and tables. YY: Data analysis and writing original draft. HS: Conceptualization, project administration. ZD: Conceptualization, project administration, supervision. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
This study adhered to the ethical guidelines of the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Hospital of Qingdao University (approval code: QYFYWZLL27495). Written informed consent was obtained from all participants and their guardians.
The authors thank Editage (https://www.editage.cn/) for English language editing.
This research received no external funding.
The authors declare no conflict of interest.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.