

 , Mengmeng Chen 1,2, Yisi Wang 1,2, Ling Han 1,2, Ai Zheng 1,2, Yali Chen 1,2,3,*
, Mengmeng Chen 1,2, Yisi Wang 1,2, Ling Han 1,2, Ai Zheng 1,2, Yali Chen 1,2,3,*
1 Department of Obstetrics and Gynecology, West China Second University Hospital, Sichuan University, 610041 Chengdu, Sichuan, China
2 Key Laboratory of Birth Defects and Related Diseases of Women and Children (Sichuan University), Ministry of Education, 610041 Chengdu, Sichuan, China
3 Department of Gynecology, Hi-Tech Zone Hospital for Women and Children, West China Second University Hospital, Sichuan University, 610095 Chengdu, Sichuan, China
Abstract
High-intensity focused ultrasound (HIFU) represents a new technology in the treatment of uterine fibroids. The curative effect of HIFU is affected by the blood supply of uterine fibroids. Oxytocin is an effective medication for promoting uterine contractions and reducing blood flow to uterine fibroids. This study aimed to evaluate the safety and efficacy of oxytocin-enhanced HIFU in treating uterine fibroids.
A systematic search of the PubMed, Embase, Cochrane Library, and Web of Science databases was conducted (up to December 14, 2024). Cohort studies reporting the impact of oxytocin on HIFU outcomes were included. A meta-analysis was performed using RevMan 5.3 software, focusing on the non-perfused volume percentage (NPV%). The NPV% is typically used to represent the effective ablated tissue volume, which is then used to calculate the ratio of the non-perfused volume to the volume of the primary fibroids after HIFU treatment.
Seven studies met the screening criteria, three of which had a primary outcome measure including NPV%. A meta-analysis showed that oxytocin significantly increased NPV% [mean difference (MD): 13.31, 95% CI: 9.17–17.44; p < 0.00001], with low heterogeneity (I2 = 26.00%). Minimal and transient side effects were reported.
Oxytocin enhances the efficacy of HIFU for uterine fibroids by increasing the NPV% and improving procedural outcomes. Nonetheless, further studies are needed to confirm the long-term benefits and safety of oxytocin in conjunction with HIFU.
The study has been registered on https://www.crd.york.ac.uk/prospero/ (registration number: CRD42024627652, registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024627652)
Keywords
- oxytocin
- high-intensity focused ultrasound
- uterine fibroids
- non-perfused volume
Uterine fibroids are the most prevalent benign tumors among reproductive-aged
women, affecting 70%–80% of this population. Uterine fibroids can cause
symptoms such as heavy menstrual bleeding, pelvic pain, and infertility, making
them the primary indication for hysterectomy [1, 2]. The conventional management
of uterine fibroids involves pharmacological interventions
(gonadotropin-releasing hormone agonists and selective progesterone receptor
modulators) and surgical approaches encompassing minimally invasive techniques
and laparotomy. Primary surgical options consist of total hysterectomy, which
results in permanent fertility loss, and myomectomy requiring postoperative
contraception for
This systematic review and meta-analysis were conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and followed the latest recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions. The protocol was prospectively registered with the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42024627652), registration link: https://www.crd.york.ac.uk/PROSPERO/view/CRD42024627652[13].
Studies were selected based on the following criteria: Inclusion criteria: (1) Studies of patients with uterine fibroids eligible for HIFU treatment. (2) Oxytocin was administered during HIFU treatment. (3) Only oxytocin was used during HIFU treatment. Exclusion criteria: (1) Duplicate publications or overlapping datasets. (2) Reviews, editorials, case reports, conference abstracts, or non-peer-reviewed articles. (3) Studies lacking a control group for comparison. (4) Non-English language publications.
A comprehensive literature search was performed across the PubMed, Embase, Cochrane Library, and Web of Science databases up to December 14, 2024. The search strategy employed a combination of medical subject headings (MeSH) and free-text keywords grounded in the PICOS principles, encompassing “leiomy (MeSH),” “fibroid,” “fibroid tumors,” “uterine fibroid,” “uterine fibroma,” “high-intensity focused ultrasound (HIFU),” “high-intensity focused ultrasound ablation,” “oxytocin,” and “Syntocinon.” The precise search syntax for each database is available in Supplementary Table 1.
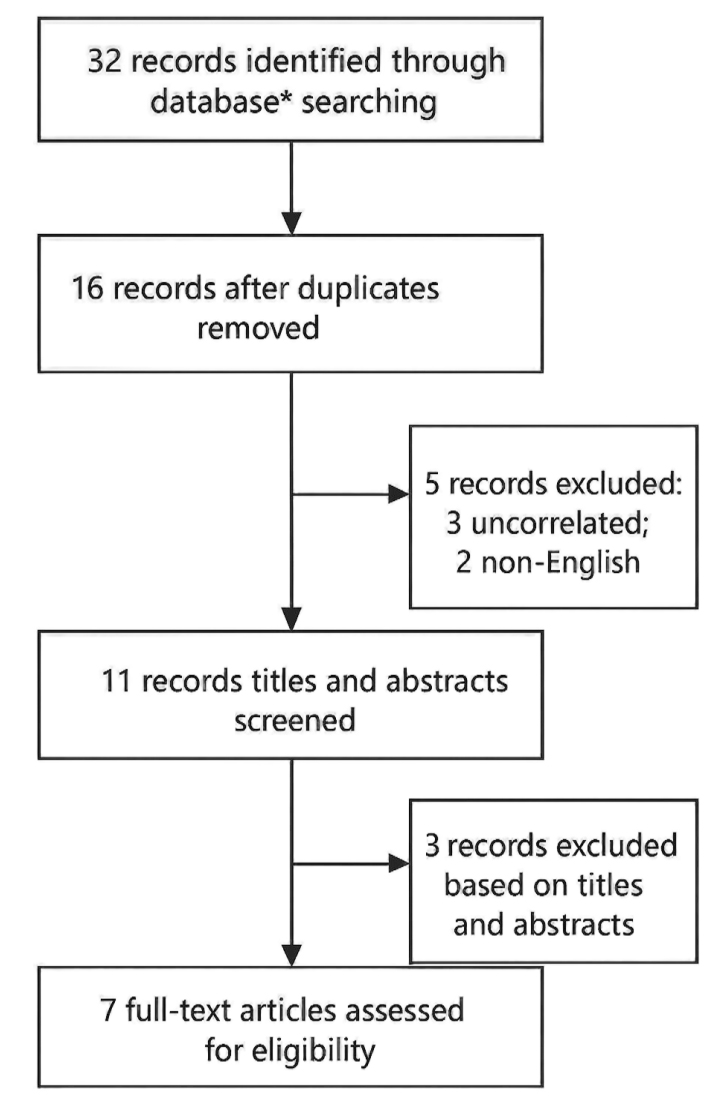
Two independent investigators (YW and MC) screened titles and abstracts, and cross-checking was performed to identify potentially eligible studies. In addition, reference lists of included articles and relevant systematic reviews were manually reviewed by two investigators (QQ and LH) to identify additional eligible studies. Any disagreements between the two parties were resolved through independent discussion with a third reviewer (AZ). The study selection process is illustrated in Fig. 1 and conforms to the PRISMA guidelines. Finally, 7 studies met the inclusion criteria, and all were cohort studies.
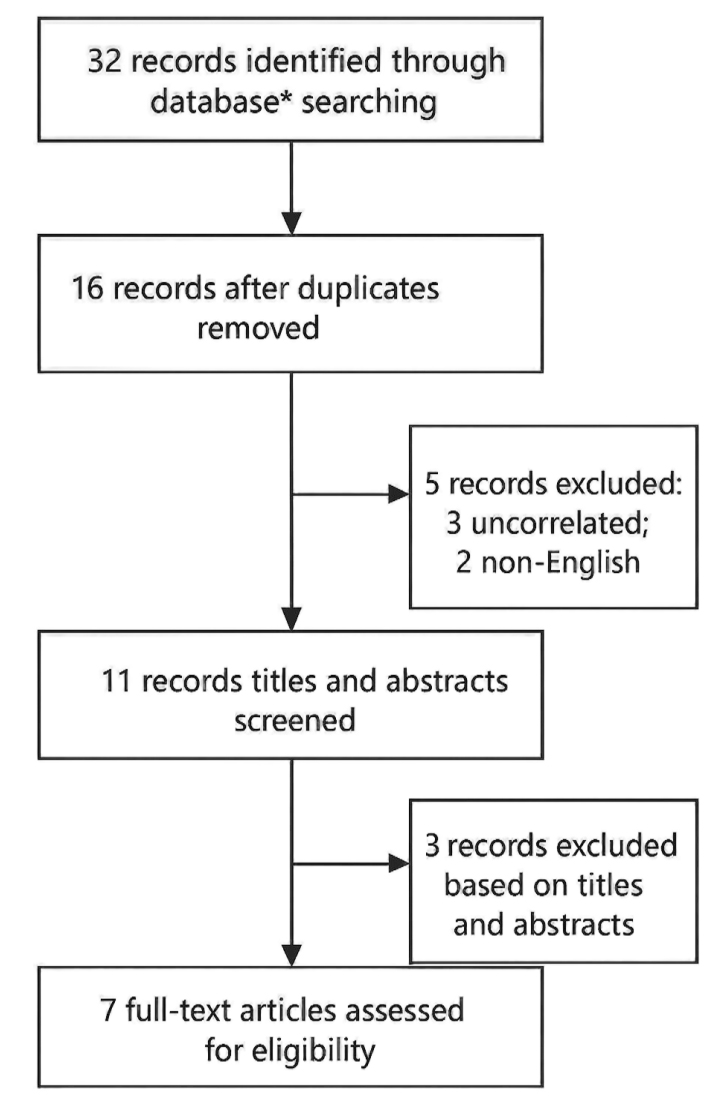 Fig. 1.
Fig. 1.
Flowchart of the article analysis criteria following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines. *PubMed (n = 10), Embase (n = 5), Web of Science (n = 13), Cochrane Library (n = 4).
Data extraction was performed independently by two reviewers (QQ and LH) using a
standardized form. Extracted variables included first author, publication year,
study design, study duration, sample size, follow-up period, and primary
outcomes. The non-perfused volume (NPV) ratio was extracted as a common efficacy
endpoint from three studies. The methodological quality of cohort studies was
assessed using the Newcastle-Ottawa scale (NOS) [14], with a score of
Analyses were conducted using Review Manager (RevMan, version 5.3; The Cochrane
Collaboration, Copenhagen, Denmark). Heterogeneity across studies was quantified
using the fixed-effects model, with I2 calculated from the mean and
standard deviation; an I2
Our literature search yielded 32 studies, of which 16 were identified as duplicates. Following the review of titles and abstracts, three studies were excluded due to irrelevance based on study design and outcomes. Full-text evaluations led to the further exclusion of three studies that did not meet the inclusion criteria related to study design, population, or intervention. Ultimately, seven studies met our inclusion criteria (Fig. 1), three of which included the outcome of interest, the NPV percentage (NPV%). All included studies were categorized as cohort studies, with their quality assessed using the NOS (Tables 1,2, Ref. [6, 9, 15, 16, 17, 18, 19]) [14]
| Study | First author, year | Method | People | Study period | Patients | Mean follow-up (months) | Primary outcome | |
| Oxytocin | Contral | |||||||
| Study 1 | Jae-Hyeok Jeong, 2016 [15] | retrospective | Korea | 2015–2016 | 39 | 118 | 6 | NPV ratio (%) |
| Volume ratio of fibroids after MRgFUS (%) | ||||||||
| Complication | ||||||||
| Re-intervention | ||||||||
| Study 2 | Yang Wang, 2016 [18] | prospective | China | 2013–2014 | 40 | - | NA | Maximum strength |
| Average transit time | ||||||||
| Time to peak strength | ||||||||
| Study 3 | Tomasz Lozinski, 2018 [16] | prospective | Poland | 2016–2017 | 51 | 105 | 15 | NPV% |
| Mean fibroid volume change% | ||||||||
| Study 4 | Simon Chun-Ho Yu, 2019 [17] | prospective | China | 2013–2017 | 9 | 24 | 24 | Adverse events |
| Symptom free | ||||||||
| Fibroid volume compared with baseline (%) median | ||||||||
| Quality of life (SF-36) at 3 months Score 100 in 5 categories | ||||||||
| Re-intervention | ||||||||
| Toleration outcome median | ||||||||
| Study 5 | Tomasz Łoziński, 2021 [6] | retrospective | Poland | 2015–2020 | 71 | 155 | 6 | NPV% |
| MRI volume cm3 | ||||||||
| Study 6 | Kimberley J. Anneveldt, 2022 [9] | prospective | Netherland | 2018–2019 | 30 | - | NA | Energy Efficiency Factor (EEF) |
| Thermal dose volume | ||||||||
| Sonication time to ablate one cm3 of fibroid tissue | ||||||||
| Adverse events | ||||||||
| Study 7 | Jakub Kociuba, 2023 [19] | retrospective | Poland | 2015–2022 | 67 | 266 | NA | Surgical interruption |
NPV, non-perfused volume; MRgFUS, Magnetic Resonance-guided Focused Ultrasound; n, number of samples; NA, not applicable; MRI, magnetic resonance imaging.
| Study | First author, year | Selection | Comparability | Outcome | Scores |
| Study 1 | Jae-Hyeok Jeong, 2016 [15] | 4 | 2 | 3 | 9 |
| Study 2 | Yang Wang, 2016 [18] | 4 | 2 | 2 | 8 |
| Study 3 | Tomasz Lozinski, 2018 [16] | 4 | 1 | 3 | 8 |
| Study 4 | Simon Chun-Ho Yu, 2019 [17] | 4 | 2 | 3 | 9 |
| Study 5 | Tomasz Łoziński, 2021 [6] | 4 | 1 | 3 | 8 |
| Study 6 | Kimberley J. Anneveldt, 2022 [9] | 4 | 2 | 2 | 8 |
| Study 7 | Jakub Kociuba, 2023 [19] | 4 | 1 | 2 | 7 |
We performed a meta-analysis to assess the impact of oxytocin on NPV% in the context of HIFU treatment for uterine fibroids. Three studies [6, 15, 16] reported NPV% as an outcome.
The pooled MD for NPV% between the oxytocin and control groups was calculated
to be 13.31 (95% CI: 9.17–17.44), demonstrating a statistically significant
positive effect of oxytocin (p
 Fig. 2.
Fig. 2.
Forest plot of NPV%. Study group: with oxytocin; control group: no oxytocin; NPV%, non-perfused volume percentage; I2, I-squared; IV, Inverse Variance; Fixed, Fixed Effects.
Regarding safety, oxytocin has demonstrated a favorable short-term safety profile in HIFU treatments for uterine fibroids. The incidence of transient adverse events (such as mild nausea and dizziness) was reported to be less than 5%, and these events can become resolved without intervention [9, 15]. In comparison, although carbetocin offers logistical advantages as a single-dose agent, a limited cohort study (n = 30) revealed that transient side effects occurred in 16.7% of patients [9]. This suggests that oxytocin is better tolerated in this context. Studies on re-intervention and quality of life assessment showed that the quality of life of the study group would be significantly improved; however, two studies on re-intervention reached opposite conclusions [15, 17].
Overall, the results demonstrated that oxytocin administration led to a significant increase in NPV% relative to the control group, thereby underscoring the potential of administering this drug to enhance the efficacy of HIFU in treating uterine fibroids. Additionally, oxytocin exhibited a favorable safety profile.
In HIFU treatment, the therapeutic efficacy is commonly quantified using the NPV%, which corresponds to the volume of tissue effectively ablated. NPV% denotes the ratio of the non-perfused volume after HIFU treatment relative to the original fibroid volume. This quantitative metric serves as a critical imaging biomarker for assessing the success of uterine fibroid ablation therapy [20, 21]. The meta-analysis showed a pooled MD of 13.31 in the NPV% between the oxytocin and control groups, with a 95% CI of 9.17–17.44. This result, combined with a low heterogeneity value (I2 = 26.00%), indicates a consistent effect of oxytocin across the studies. The statistically significant improvement in NPV% underscores the enhanced thermal ablation efficiency associated with oxytocin administration. A higher NPV% correlates with increased tissue necrosis, improved clinical outcomes, and potential symptom relief, establishing this metric as a critical marker of treatment success in HIFU therapy [6, 15, 16]. Funaki et al. [22] noted that the efficacy of HIFU treatment for uterine fibroids is influenced by the vascularization and blood flow within the fibroids. Oxytocin enhances thermal efficiency by reducing blood perfusion, which is achieved through uterine smooth muscle contraction, ultimately decreasing vascular supply and mitigating the cooling effect of high blood flow [18, 22, 23]. This reduction in perfusion facilitates more effective energy deposition, as evidenced by the increased NPV% and reduced energy requirements observed in the analyzed studies. These physiological effects not only boost HIFU efficacy but also address a significant limitation related to outcome variability caused by fibroid vascularization [16].
Oxytocin not only increases the NPV% but also significantly shortens treatment duration and reduces procedural interruptions. These subsequent shorter treatment times improve patient comfort and facilitate greater efficiency in the utilization of MRI-guided HIFU systems, potentially reducing the overall cost of the procedure [15]. Studies consistently reported fewer instances of treatment discontinuation in the oxytocin group, likely due to decreased discomfort and improved ablation efficiency. However, there was notably no clear consensus in the studies on the timing and dosage of oxytocin use, which is related to the habits of clinical workers.
The safety profile of uterine stimulants used in HIFU treatments is well-established. Temporary side effects, such as mild nausea or dizziness, are typically self-limiting and easily managed [9]. Moreover, no severe or long-term adverse effects have been reported. These benefits make uterine stimulants a practical and effective adjunct to HIFU therapy, enhancing both efficacy and usability. Furthermore, the implementation of personalized treatment protocols based on factors such as fibroid vascularity—classified by the Funaki system [24]—has further improved treatment effectiveness, especially for challenging cases such as Funaki type 3 fibroids [9, 17]. These advancements highlight the importance of tailoring HIFU treatments to individual patient characteristics for optimal results.
In addition, advanced imaging techniques, especially a 3-Tesla (3T) MRI scanning system, markedly aid in the use of uterotonic agents, such as oxytocin, in magnetic resonance (MR)-guided HIFU treatment of uterine fibroids [6]. High-resolution imaging allows for detailed vascular analysis and accurate patient selection for uterotonic-enhanced MR-HIFU treatment [6, 25]. Dynamic contrast-enhanced MRI has also emerged as a robust predictor of treatment outcomes, evidenced by an improved NPV ratio with the use of uterotonic agents [9, 26]. These advancements underscore the critical role of imaging in maximizing the efficacy and safety of oxytocin-enhanced MR-HIFU for the treatment of uterine fibroids.
This systematic review and meta-analysis demonstrate that oxytocin significantly enhances the efficacy of HIFU treatment for uterine fibroids. Moreover, by improving the NPV%, reducing procedural duration, and decreasing treatment discontinuation rates, administering oxytocin serves as a valuable adjunctive approach to optimize this non-invasive therapy [19].
Furthermore, misoprostol, a uterotonic agent, has likewise been investigated as a treatment for uterine fibroids using MR-HIFU; Łoziński et al. [6, 10] highlighted distinct effects of misoprostol/diclofenac and oxytocin in enhancing MR-HIFU outcomes. The findings by Łoziński et al. [6, 10] showed that the misoprostol/diclofenac combination achieved a higher immediate NPV than the oxytocin group, reduced sonication time, and improved procedural efficiency. However, the misoprostol/diclofenac combination was associated with the lowest reduction in fibroid volume six months post-treatment. In contrast, oxytocin, although slightly less effective in achieving immediate NPV, resulted in the greater long-term reduction in fibroid volume, likely due to the sustained uterotonic effects of oxytocin. These findings suggest that misoprostol/diclofenac may optimize immediate procedural outcomes, whereas oxytocin may improve support for long-term fibroid regression. However, due to the limited number of studies on the application of misoprostol in MR-HIFU, the safety and efficacy of misoprostol require further clinical data for validation. Therefore, tailored pharmacological strategies could play a critical role in maximizing the efficacy of MR-HIFU treatment.
Despite the promising findings, the safety evaluation of uterotonics in HIFU therapy warrants cautious interpretation due to limitations in the current evidence. Most studies have primarily focused on short-term side effects, reporting mild and transient adverse events such as nausea or dizziness, which were self-limiting and manageable [9, 15]. However, the heterogeneity in adverse event reporting, including follow-up durations, limits a comprehensive risk assessment. Additionally, small sample sizes and limited patient diversity likely underestimate rare or delayed adverse events. Future research should standardize adverse event monitoring, include larger and more diverse cohorts, and extend follow-up periods to improve characterization of both acute and long-term safety profiles of uterotonics in HIFU therapy [9].
To our knowledge, this represents the first systematic review and meta-analysis to evaluate the safety and efficacy of oxytocin in HIFU therapy for uterine fibroids. By synthesizing existing evidence, this study highlights the potential of oxytocin to improve therapeutic outcomes, including enhanced thermal efficiency and NPV%. Nevertheless, several limitations must be acknowledged. The scarcity of available studies limits the analysis, as evidenced by the lack of randomized controlled trials (RCTs) and the reliance on retrospective or small-scale research. Heterogeneity in dosing, patient selection, and treatment protocols further limits the generalizability of the findings. There are no clear standards regarding the timing, mode, and dose of oxytocin administration. These gaps highlight the need for robust, prospective studies to confirm these results.
Future investigations should focus on optimizing the dosage and timing of oxytocin administration, as well as evaluating its effectiveness in specific patient subgroups, particularly those with highly vascularized fibroids. Advanced imaging techniques, such as perfusion-weighted MRI, can provide critical insights into real-time changes in fibroid vascularity during HIFU, paving the way for more personalized treatments [6]. Moreover, large-scale randomized trials with prolonged follow-ups are crucial for validating these findings and establishing robust clinical guidelines. Similarly, further trials are needed to assess the efficacy and safety of misoprostol in MR-HIFU, particularly its potential to enhance immediate procedural efficiency and support long-term fibroid regression.
Oxytocin significantly improves the efficacy of HIFU treatment for uterine fibroids by increasing NPV%, improving procedural efficiency, and maintaining a favorable safety profile. These findings provide a solid foundation for clinical application while underscoring the need for further research to optimize the use of HIFU and confirm its long-term benefits. Future studies should focus on determining the optimal dosage and administration protocols, as well as identifying specific patient subgroups that may derive the greatest benefit from this adjunctive treatment.
HIFU, high-intensity focused ultrasound; NPV%, non-perfused volume percentage; UAE, uterine artery embolization; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses; RCTs, randomized controlled trials; MeSH, Medical Subject Headings; NOS, Newcastle-Ottawa scale; MD, mean difference; MRgFUS, Magnetic Resonance-guided Focused Ultrasound; n, number of samples; FDA, Food and Drug Administration; MRI, magnetic resonance imaging; 3T, 3-Tesla.
The data underlying this study are available in a public, open-access repository. Data can also be made available upon reasonable request. All relevant data have been included in the article or uploaded as supplementary information.
Study design: QQ, MC, YC. Literature search: QQ, MC, YW, LH. Statistical analysis: QQ, YW, AZ. All authors contributed to critical revision of the manuscript for important intellectual content. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Not applicable.
We would like to express our gratitude to all those who helped us during the writing of this manuscript.
This research received no external funding.
The authors declare no conflict of interest.
During the preparation of this manuscript, the authors utilized ChatGPT-3.5 solely for grammar and language polishing. The authors thoroughly reviewed, edited, and revised the manuscript and take full responsibility for its content.
Supplementary material associated with this article can be found, in the online version, at https://doi.org/10.31083/CEOG40247.
References
Publisher’s Note: IMR Press stays neutral with regard to jurisdictional claims in published maps and institutional affiliations.